CONTEXTO O número de idosos (com idade ≥ 65 anos) em todo o mundo deverá triplicar até 2050, sendo que um quarto desses indivíduos estará na faixa etária dos “idosos longevos” (com idade > 85 anos).(1) A prevalência de doenças pulmonares crônicas e de comorbidades que podem influenciar os testes de função pulmonar aumenta com o envelhecimento. Conhecer os efeitos fisiológicos da senescência no sistema respiratório é fundamental para evitar o subdiagnóstico ou o sobrediagnóstico de doenças respiratórias em idosos.
VISÃO GERAL Um homem de 77 anos, com carga tabágica = 50 anos-maço — ele havia deixado de fumar 10 anos antes — insuficiência cardíaca (fração de ejeção do ventrículo esquerdo = 36%) e fibrilação atrial, apresentou dispneia progressiva (3 pontos na escala modificada do Medical Research Council) após uma infecção do trato respiratório inferior que foi tratada em casa. A radiografia de tórax mostrou pequenas opacidades lineares no lobo inferior direito. O paciente recebeu diagnóstico de DPOC com base nos seguintes dados: a) VEF1/CVF < 0,7 (porém acima do limite inferior da normalidade); b) VEF1/CV “lenta” abaixo do limite inferior da normalidade; c) redução limítrofe do FEF25-75%, com algum “scooping” expiratório (concavidade da alça expiratória); d) aumento discreto do VR; e) ligeira redução da DLCO. O formoterol inalatório não melhorou a dispneia; causou efeitos colaterais indesejáveis (palpitações e tontura) e, portanto, foi suspenso. A dispneia cedeu após algumas semanas de fisioterapia respiratória para a eliminação de secreções.
Há relação entre o envelhecimento e a perda tanto da retração elástica pulmonar como de ligações alveolares às pequenas vias aéreas, ambas as quais contribuem para a diminuição dos fluxos expiratórios e, consequentemente, do VEF1 e FEF25-75% (a-c acima). Fluxos meso e tele-expiratórios baixos podem criar uma ligeira concavidade na curva de fluxo expiratório (c). O aumento do volume de relaxamento do sistema respiratório e a tendência ao fechamento das vias aéreas em baixos volumes pulmonares causam o aumento da capacidade residual funcional e do VR (d), respectivamente. A CPT pode permanecer inalterada ou diminuir em decorrência da maior rigidez da parede torácica, reduzindo a capacidade inspiratória e a CV.(2) Como as pequenas vias aéreas tendem a se fechar mais cedo durante uma manobra expiratória forçada do que durante uma manobra expiratória “lenta”, a CVF diminui mais do que a CV; assim, a relação VEF1/CV diminui mais do que a relação VEF1/CVF (a-b acima).(3) Como o volume em que as pequenas vias aéreas começam a se fechar durante a expiração aumenta mais do que a capacidade residual funcional, as desigualdades na distribuição da ventilação podem diminuir a eficiência das trocas gasosas pulmonares. Dilatação dos espaços aéreos sem destruição alveolar distinta e densidade reduzida dos bronquíolos membranosos sugerem a coalescência de alvéolos menores e maiores, reduzindo a superfície funcional para trocas gasosas e, ao mesmo tempo, aumentando áreas de alta relação ventilação-perfusão.(2) O corolário é a redução, em virtude da idade, da DLCO (e) e da PaO2, bem como o aumento do gradiente alveoloarterial de oxigênio (Tabela 1).
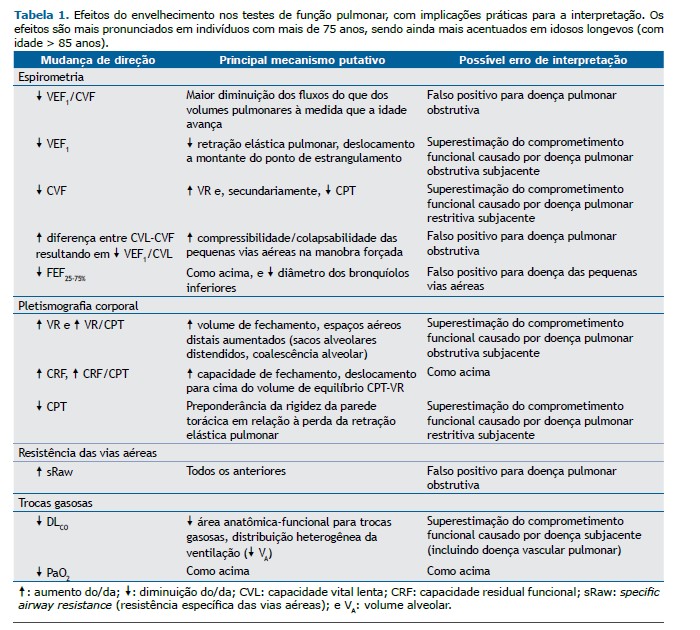
Várias alterações fisiológicas relacionadas ao envelhecimento podem simular as anormalidades induzidas pela doença das vias aéreas, incluindo fluxos expiratórios baixos, volumes pulmonares operantes aumentados e desigualdades na distribuição da ventilação. Por outro lado, a predominância da rigidez da parede torácica em relação à perda da retração elástica pulmonar pode gerar preocupações injustificadas a respeito de restrição, particularmente na presença de obesidade moderada a grave.(4) O fato de que os valores de referência são menos precisos nos extremos de idade complica ainda mais esse cenário.(5) É preciso muito cuidado para evitar o sobrediagnóstico de doença respiratória (ou a superestimação do comprometimento causado por doenças preexistentes) em idosos.
REFERÊNCIAS 1. National Institutes of Health. National Institute on Aging [homepage on the Internet]; Bethesda: National Institute on Aging [updated: 2011 Oct; cited: 2022 Jul 19]. Global health and aging: Preface. [Adobe Acrobat document; 32p.]. Available from: https://www.nia.nih.gov/sites/default/files/2017-06/global_health_aging.pdf
2. Neder JA, Berton DC, O’Donnell DE. The Lung Function Laboratory to Assist Clinical Decision-making in Pulmonology: Evolving Challenges to an Old Issue. Chest. 2020;158(4):1629-1643. https://doi.org/10.1016/j.chest.2020.04.064
3. Saint-Pierre M, Ladha J, Berton DC, Reimao G, Castelli G, Marillier M,et al. Is the Slow Vital Capacity Clinically Useful to Uncover Airflow Limitation in Subjects With Preserved FEV1/FVC Ratio?. Chest. 2019;156(3):497-506. https://doi.org/10.1016/j.chest.2019.02.001
4. Marillier M, Bernard AC, Reimao G, Castelli G, Alqurashi H, O’Donnell DE, et al. Breathing at Extremes: The Restrictive Consequences of Super- and Super-Super Obesity in Men and Women. Chest. 2020;158(4):1576-1585. https://doi.org/10.1016/j.chest.2020.04.006
5. Neder JA, Berton DC, O’Donnell DE. Lung function: what constitutes (ab)normality?. J Bras Pneumol. 2022;48(2):e20220096. https://doi.org/10.36416/1806-3756/e20220096











 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket