ABSTRACT
Objective: To investigate factors that influence or promote disbelief and negative attitudes toward COVID-19. Methods: This was cross-sectional study involving 544 males and females = 18 years of age in Greece between December of 2020 and January of 2021. All participants were informed about the purpose of the study, protection of anonymity, and volunteer participation. Participants completed an online anonymous 40-item questionnaire. Analysis of data included the identification of correlations and use of t-tests and ANOVA. Results: The level of knowledge regarding COVID-19 transmission routes, manifestations, and prevention was high in our sample. Women appeared to have a more positive attitude toward COVID-19 prevention and management than did men (p = 0.032 and p = 0.018, respectively). Younger people (18-30 years of age) seemed to deny the validity of scientific data and mass media reports about ways to deal with the pandemic more commonly than did those > 30 years of age (p = 0.003 and p = 0.001, respectively). People who resided in cities more commonly believed in scientific announcements than did those living in villages (p = 0.029). Conclusions: In order to minimize cases of denial of and disbelief in COVID-19 and to promote vaccination, a series of actions are required. Governments should implement a series of measures to contain the disease, taking into consideration the psychological and social aspects of those policies.
Keywords:
Vaccination; COVID-19; Health knowledge, attitudes, practice.
RESUMO
Objetivo: Investigar fatores que influenciam ou promovem a descrença e atitudes negativas em relação à COVID-19. Métodos: Estudo transversal envolvendo 544 homens e mulheres com ≥ 18 anos de idade na Grécia entre dezembro de 2020 e janeiro de 2021. Todos os participantes foram informados sobre o objetivo do estudo, proteção do anonimato e participação voluntária. Os participantes responderam a um questionário on-line anônimo com 40 itens. A análise dos dados incluiu a identificação de correlações e o uso de testes t e ANOVA. Resultados: O nível de conhecimento sobre as vias de transmissão, manifestações e prevenção da COVID-19 foi alto em nossa amostra. As mulheres pareceram ter uma atitude mais positiva em relação à prevenção e manejo da COVID-19 do que os homens (p = 0,032 e p = 0,018, respectivamente). As pessoas mais jovens (18-30 anos de idade) pareceram negar mais a validade dos dados científicos e reportagens da mídia sobre as formas de lidar com a pandemia do que aquelas com > 30 anos de idade (p = 0,003 e p = 0,001, respectivamente). As pessoas que residiam em cidades grandes acreditavam mais nos pronunciamentos científicos do que as que residiam em vilas (p = 0,029). Conclusões: Para minimizar o número de casos de negação e descrença em relação à COVID-19 e promover a vacinação, é necessária uma série de ações. Os governos devem implementar uma série de medidas para conter a doença, levando em consideração os aspectos psicológicos e sociais dessas políticas.
Palavras-chave:
Vacinação; COVID-19; Conhecimentos, atitudes e prática em saúde.
INTRODUÇÃO Em dezembro de 2019, vários casos de infecções do trato respiratório inferior de causa desconhecida foram relatados na cidade de Wuhan, província de Hubei, na China. Em 7 de janeiro de 2020, uma nova cepa de coronavírus foi identificada como a causa dessas infecções e recebeu um nome provisório: 2019-nCoV. O aumento contínuo do número de novos casos em todo o mundo obrigou a OMS a anunciar a caracterização da doença como pandemia cerca de dois meses após a identificação da cepa infecciosa.(1)
Recentemente, os cientistas enfrentaram situações pandêmicas ameaçadoras causadas por diferentes cepas da família Coronavírus, as quais conseguiram conter com sucesso. Especificamente, a síndrome respiratória do Oriente Médio foi relatada pela primeira vez na Arábia Saudita em setembro de 2012, e, segundo a OMS, 2.519 casos e 866 mortes foram relatados em todo o mundo até janeiro de 2020. A síndrome respiratória aguda grave foi relatada pela primeira vez na Ásia em fevereiro de 2003 e se espalhou rapidamente por 26 países antes de ser contida após aproximadamente quatro meses. Durante esse período, mais de 8.000 pessoas ficaram doentes e 774 morreram. Desde 2004, não foi relatado nenhum caso dessa síndrome.(2)
Do início da pandemia de COVID-19 até a redação deste artigo, observou-se em todo o mundo uma atitude de negação e descrença em relação à doença, juntamente com um questionamento extremo sobre as medidas preventivas, as manifestações da doença e o manejo de casos suspeitos e confirmados. De acordo com os resultados de um estudo global,(3) 13% dos americanos não acreditavam que a COVID-19 fosse real, sendo as taxas mais altas de descrença na doença foram encontradas na Turquia e Polônia (22% da população), no Egito e Arábia Saudita (19%), seguidos pela Nigéria e Grécia (17%).
A análise dos fatores e motivos da adoção de uma atitude negativa em relação à COVID-19 é uma tarefa complicada e tediosa. Os motivos que levaram as pessoas a negar ou minimizar a existência e evolução da pandemia estão principalmente relacionados a fatores psicológicos, pessoais, sociais e políticos. A primeira fase desse fenômeno começou com a publicação de dados epidemiológicos, criando uma sensação de ameaça iminente. Uma parte das pessoas assumiu uma postura negacionista como mecanismo inato de sobrevivência contra as dificuldades futuras a fim de lidar com a sobrecarga de informações e o constante bombardeio de terminologia médica.(4-6)
Outro parâmetro importante que contribui para a espiral desse fenômeno é a obrigatoriedade do uso de equipamentos de proteção individual (EPI) e a restrição das atividades pessoais e sociais. A introdução dos EPI preventivos causou sentimentos de confinamento, angústia e ansiedade que se traduziram em descrença, possíveis violações de direitos humanos e explosões de comportamentos reativos. A obrigatoriedade do uso de EPI foi explorada por muitos como instrumento de oposição política às iniciativas governamentais, resultando em uma oportunidade de promoção de interesses políticos.(7,8)
Restrições constantes, longos períodos de isolamento social e consecutivas ondas pandêmicas em grande escala causaram o adiamento ou cancelamento de atividades importantes como viagens, excursões, eventos esportivos e comemorações, gerando sentimentos de pesar e indignação na população, o que por sua vez levou as pessoas a minimizar a doença e assumir uma visão negacionista da gravidade da pandemia e da utilidade das medidas restritivas.(9,10)
O objetivo do presente estudo foi investigar os fatores que influenciam ou promovem a descrença e as atitudes negativas em relação à COVID-19.
MÉTODOS O presente estudo teve um desenho transversal. O motivo dessa escolha foi a credibilidade dos resultados produzidos, pois esse desenho é considerado o mais adequado para a coleta de dados de muitos participantes. O estudo foi composto por uma amostra de conveniência com 544 participantes adultos (≥ 18 anos de idade). Inicialmente, 600 participantes manifestaram interesse em fazer parte do estudo, resultando em uma taxa de resposta de 90,67%. Os participantes foram inicialmente informados sobre o objetivo da pesquisa, proteção do anonimato e participação voluntária. Em seguida, os participantes foram solicitados a responder a um questionário on-line anônimo e autoaplicável. Este estudo foi realizado entre 1º de dezembro de 2020 e 31 de janeiro de 2021.
Para garantir a validade do conteúdo do questionário, revisou-se a literatura grega e internacional relevante. Após uma leitura crítica meticulosa da literatura relevante, não foram encontradas ferramentas de medição que avaliassem o conhecimento das pessoas sobre a COVID-19 e sua crença ou não de que a doença era real. Como resultado, desenvolvemos um questionário em grego e realizamos um teste piloto com 15 pessoas para avaliar a validade e confiabilidade do questionário.(11)
A consistência interna (confiabilidade) de um questionário representa até que ponto as subpartes do questionário medem a mesma característica. A avaliação da confiabilidade é extremamente útil, pois avalia a consistência das questões e, por extensão, das respostas.
A validade de um questionário representa até que ponto o questionário mede o que foi projetado para medir. As medições precisam ser relevantes para as características que o pesquisador deseja estudar. Os diferentes aspectos de validade examinados em nosso questionário foram a validade de face e de conteúdo.
O presente estudo foi realizado de acordo com os padrões dos comitês de ética em pesquisa institucional e nacional e em conformidade com a Declaração de Helsinque de 1964 e suas alterações posteriores ou padrões éticos equivalentes. O estudo foi projetado e conduzido de acordo com os princípios éticos estabelecidos pela Universidade da Tessália, na Grécia (declaração de aceitação n. 77).
A estrutura final do questionário incluiu 8 questões sobre conhecimento sobre a transmissão, manifestações e prevenção da COVID-19; 10 questões sobre fontes de informação; 10 questões sobre a confiança nos dados científicos relacionados à doença e a aceitação desses dados; 10 questões sobre a influência do meio social na crença/descrença na doença; e 10 questões sobre atitudes e preferências em relação à vacinação. As respostas às últimas 30 questões foram pontuadas em uma escala Likert de cinco pontos, variando de 1 (discordo inteiramente/totalmente) a 5 (concordo inteiramente/totalmente). O coeficiente alfa de Cronbach foi de 0,68, mostrando uma consistência interna limítrofe.
No presente estudo, foram empregadas estatísticas descritivas e inferenciais. As variáveis descritivas foram expressas como frequências absolutas e relativas ou médias e desvios-padrão. A estatística inferencial foi utilizada considerando a importância dos resultados; por isso, foram realizados testes independentes em conjunto com testes paramétricos, já que os resultados apresentaram distribuição normal. Mais especificamente, o teste t de Student foi aplicado para variáveis binárias, pois se pressupõe que amostras maiores tenham distribuição normal; para variáveis com três ou mais valores, ANOVA foi escolhida para controlar o impacto de duas ou mais variáveis independentes na variável dependente. O nível de significância bicaudal adotado foi de p ≤ 0,05. A análise dos dados foi realizada com o programa IBM SPSS Statistics, versão 25.0 (IBM Corporation, Armonk, NY, EUA).
RESULTADOS A porcentagem de homens e mulheres na amostra foi de 17,8% e 82,0%, respectivamente. No que tange à distribuição etária, 50,6% estavam na faixa etária de > 30 anos, enquanto 49,4% estavam na faixa etária de 18 a 30 anos. A maioria dos participantes era de nacionalidade grega (97,6%). Quanto à escolaridade, a maioria dos participantes possuía ensino superior completo/pós-graduação (43,0%); dentre eles, 17,5% e 2,2% possuíam mestrado e doutorado, respectivamente. A maioria dos participantes estava empregada (90,3%), e 39,0% relataram trabalhar no setor privado. A taxa de desemprego era de 9,7%. Quanto ao estado civil, 30,7% eram casados, 65,1% eram solteiros, 3,3% eram divorciados e 0,9% era viúvo. Por fim, 82,4% residiam em cidades grandes, 9,7%, em cidades pequenas, e 7,9%, em vilas.
Quanto ao conhecimento sobre a COVID-19, a porcentagem geral de acertos foi de 89,1%. Especificamente, as questões sobre os sintomas da COVID-19 foram respondidas corretamente por 93,9% dos participantes, assim como as sobre as vias de transmissão, por 97,4%; as sobre as características clínicas dos pacientes assintomáticos, por 97,6%; as sobre o período de incubação, por 93,6%; as sobre o tratamento, por 66,7%; as sobre a prevenção, por 68,2%; as sobre o reconhecimento dos sintomas de alerta, por 99,1%; e as sobre o diagnóstico da doença, por 96,3%. Uma diferença estatisticamente significativa foi encontrada para a questão sobre se havia tratamento específico para a doença: 68,6% das mulheres e 57,7% dos homens responderam corretamente que não havia tratamento específico. Além disso, notamos que quanto maior a escolaridade dos respondentes, maior a probabilidade de responderem corretamente a essa questão, ou seja, não há tratamento específico. Quanto à pergunta sobre a média de dias transcorridos entre a exposição a um caso confirmado de COVID-19 e o início dos sintomas, observamos uma correlação estatisticamente significativa com a idade, pois 96,3% dos respondentes com > 30 anos de idade responderam corretamente que os sintomas começariam, em média, 5-6 dias após o contato, em comparação com 3,7% daqueles com 18 a 30 anos, que responderam 22-23 dias após o contato. Na questão sobre os sintomas da COVID-19, “residir em cidades grandes” ou “residir em cidades pequenas” apresentaram correlação positiva com a resposta “perda de peso não é um dos sinais clínicos da doença” (em 94,6% e 96,2% dos respondentes, respectivamente), o mesmo não acontecendo com “residir em vilas”.
A Tabela 1 apresenta as diferenças estatisticamente significativas quanto às opiniões e atitudes em relação à COVID-19 entre homens e mulheres. Em geral, as mulheres obtiveram informações sobre a doença por meio da mídia mais do que os homens e acreditavam mais nos pronunciamentos científicos, embora acreditassem que as orientações para o tratamento e recuperação da doença não eram claras. Além disso, as mulheres seguiram mais as recomendações de proteção durante as medidas restritivas e estavam mais preocupadas com os efeitos colaterais das vacinas. Quanto aos homens, eles mostraram maior propensão a aceitar dados de estudos científicos realizados no exterior, por considerá-los de maior validade.

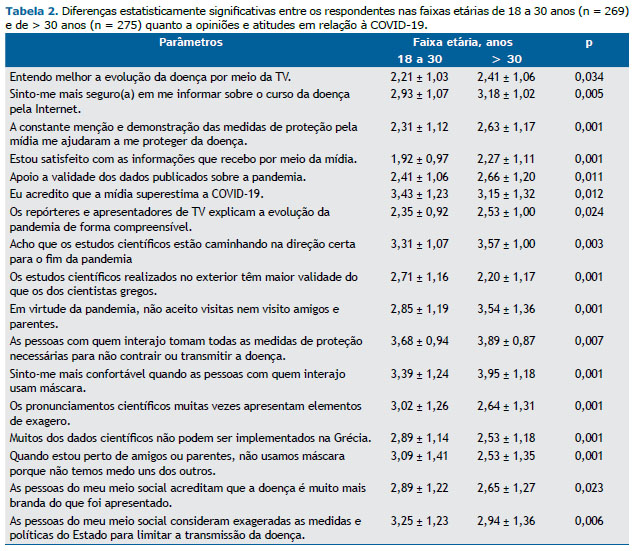
A Tabela 2 apresenta as diferenças estatisticamente significativas quanto às opiniões e atitudes em relação à COVID-19 entre as duas faixas etárias estudadas (18-30 anos e > 30 anos). Em geral, os participantes na faixa etária de > 30 anos obtiveram informações sobre a doença por meio da mídia mais do que aqueles na faixa de 18 a 30, apoiavam mais a validade dos dados publicados e acreditavam mais que os estudos científicos estavam caminhando na direção certa para o fim da pandemia. Além disso, seguiram mais as recomendações de proteção durante as medidas restritivas. Quanto àqueles na faixa etária de 18 a 30 anos, com maior frequência apresentaram opiniões e atitudes negativas em relação às informações fornecidas pela mídia e aos pronunciamentos científicos, desconsiderando os estudos científicos realizados na Grécia. Foram mais descuidados em seguir as recomendações de proteção e as medidas restritivas, e o meio social influenciou mais na sua negação e descrença em relação à gravidade da COVID-19.
Quanto ao nível de escolaridade, constatamos que quanto maior esse nível, maior a variação nas taxas de confiança; as pessoas com ensino superior, exceto aquelas com doutorado, afirmaram que confiam na comunidade científica em relação às diretrizes de prevenção da doença, que acreditam que os estudos científicos estão caminhando na direção certa para o fim da pandemia, que os pronunciamentos científicos são muito exagerados e que a maioria dos dados científicos não pode ser implementada na Grécia. Também cumprem os regulamentos e não aceitam visitantes nem visitam amigos e parentes.
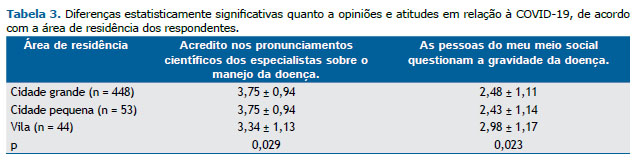
As pessoas que residiam em cidades grandes ou pequenas mostraram maior receptividade aos pronunciamentos científicos dos especialistas sobre o manejo da doença do as que residiam em vilas. Por outro lado, as pessoas que residiam em áreas rurais foram mais influenciadas pelo meio social quanto à gravidade da doença (Tabela 3).
DISCUSSÃO O presente estudo tenta definir os fatores que levam as pessoas da comunidade à negação e descrença em relação à COVID-19. A atitude das pessoas em relação a problemas de saúde está relacionada ao seu conhecimento sobre o agente infeccioso, sua escolaridade, seu estado psicoemocional e suas fontes de informação, bem como à forma como os fatos estão sendo divulgados e suas experiências pessoais anteriores. Para investigar minuciosamente a hipótese da pesquisa e os motivos mencionados acima, examinamos o conhecimento, fontes de informação e atitudes dos participantes sobre a COVID-19, bem como a influência do meio social em sua crença ou não de que a doença era real.
O nível de conhecimento sobre a COVID-19 entre os respondentes foi muito alto, com 89,1% deles respondendo corretamente às questões sobre as vias de transmissão, a prevenção e as características clínicas da doença. Um estudo semelhante de Chen et al.(12) relatou altas taxas de respostas corretas sobre os sintomas da doença, como tosse (99,5%), febre (96,0%), transmissão por gotículas (99,5%), transmissão aérea (81,1%) e transmissão por meio de contato direto (92,3%). Um alto nível de conhecimento sobre proteção contra a COVID-19 também foi documentado por Siddiqui et al.,(7) que relataram que 84% de sua amostra conhecia a técnica correta de lavagem das mãos, 82% sabiam que a doença pode ser transmitida pelo aperto de mão e 79% sabiam que deveriam manter uma distância de pelo menos um metro de outras pessoas.
O presente estudo e os estudos de Chen et al.(12) e Siddiqui et al.(7) concluíram que o nível de conhecimento das pessoas sobre prevenção, sinais clínicos e vias de transmissão da COVID-19 é particularmente alto. Esse aumento do conhecimento muito provavelmente se deve aos esforços dos profissionais de saúde para fornecer às pessoas informações válidas e científicas, como os altos níveis de morbidade e mortalidade por COVID-19 em todo o mundo e a necessidade de proteção das pessoas.
Hoje, é muito fácil acessar e divulgar informações. A mídia e a internet parecem desempenhar um papel importante na informação do público sobre problemas de saúde. Suas características dinâmicas contribuem amplamente para moldar as opiniões e atitudes das pessoas em relação a várias doenças e sua prevenção. (13-15)
No que tange às fontes de informação, as mulheres acreditavam que a constante menção e demonstração das medidas preventivas pela mídia as ajudaram bastante a se proteger da doença, em contraste com os homens. Ao mesmo tempo, as pessoas com > 30 anos de idade pareceram entender melhor a evolução da doença por meio da televisão e se sentir mais seguras em se informar sobre o curso da doença pela Internet, em contraste com aquelas com 18 a 30 anos, que acreditavam que a mídia superestima a COVID-19.
Na maioria dos países, a televisão é o meio de informação mais popular, pois o tempo médio em frente à TV é de duas horas(16) Nos últimos anos, o rápido avanço da tecnologia trouxe mudanças importantes na forma como crianças e adolescentes vivem e se informam. A posse de um computador e o acesso à internet são agora mais fáceis do que nunca, e, juntamente com o uso generalizado de dispositivos inteligentes, as pessoas têm a oportunidade de receber informações validadas rapidamente.
Observou-se o amplo uso da Internet como principal fonte de informações sobre a COVID-19. De acordo com o presente estudo, o conhecimento obtido por meio da mídia é mais aceito por pessoas com > 30 anos de idade do que por aquelas com 18 a 30 anos. Um estudo de Dkhar et al.(17) sobre o conhecimento das pessoas sobre a COVID-19 menciona que 89% da população da amostra utilizava a Internet como fonte de informação. O interesse dos jovens em buscar informações médicas on-line provavelmente está associado ao fato de estarem mais familiarizados com a Internet e, ao mesmo tempo, de a utilizarem como ferramenta para a maioria, senão todas, as atividades cotidianas como educação, compras e entretenimento.
Diversos cientistas acreditam que a rápida disseminação de informações e, principalmente, a publicação de protocolos de pesquisa sobre a prevenção, tratamento e abordagens diagnósticas da doença contribuíram para a preparação imediata dos profissionais de saúde e a aceitação mais rápida da doença nas populações de todo o mundo.(18) No entanto, o grande volume de informações durante a pandemia parece levar as pessoas à confusão e a becos sem saída. Parte das evidências médicas é ambígua, promovendo mensagens contraditórias. Estudos e práticas pouco claras e não comprovadas cientificamente são aceitos por um grupo de pessoas que estimulam impressões negativas, minimizam a doença e cultivam dúvidas para cumprir objetivos pessoais, políticos e econômicos.(19)
O presente estudo mostra que o nível de conhecimento sobre as vias de transmissão, manifestações e prevenção da COVID-19 foi alto em nossa amostra. As mulheres pareceram confiar mais nas informações sobre a prevenção e manejo da COVID-19 do que os homens. As pessoas mais jovens mostraram menor propensão a acreditar na validade dos dados científicos e reportagens da mídia sobre as formas de lidar com a pandemia, e as pessoas que residiam em cidades grandes apresentaram maior propensão a acreditar nos pronunciamentos científicos do que as que residiam em vilas.
Para minimizar o número de casos de negação e descrença em relação à COVID-19, é necessária uma série de ações. Os governos devem implementar uma série de medidas para conter a doença, levando em consideração os aspectos psicológicos e sociais dessas políticas. Os pronunciamentos e transmissões científicas devem ser simples, claros e precisos para evitar a promoção de mensagens confusas. A mídia deve informar as pessoas sobre os atuais problemas de saúde pública sem qualquer viés, opiniões pessoais ou práticas de persuasão.
AGRADECIMENTOS Gostaríamos de agradecer aos respondentes a participação neste estudo.
CONTRIBUIÇÕES DOS AUTORES AV: conceituação (liderança); curadoria de dados (igual); análise formal (igual); aquisição de financiamento (igual); investigação (igual); metodologia (liderança); administração de projeto (igual); recursos (igual); software (igual); supervisão (liderança); validação (igual); visualização (igual); redação do rascunho original (igual); revisão e edição do manuscrito (igual). NAP: conceituação (igual); curadoria de dados (igual); análise formal (suporte); aquisição de financiamento (suporte); investigação (igual); metodologia (suporte); administração de projeto (igual); recursos (suporte); software (suporte); supervisão (igual); validação (suporte); visualização (igual); redação do rascunho original (suporte); revisão e edição do manuscrito (suporte). AT: conceituação (igual); curadoria de dados (igual); análise formal (igual); aquisição de financiamento (suporte); investigação (igual); metodologia (suporte); administração de projeto (igual); recursos (igual); software (igual); supervisão (suporte); validação (igual); visualização (igual); redação do rascunho original (suporte); revisão e edição do manuscrito (suporte). DP: conceituação (igual); curadoria de dados (igual); análise formal (igual); aquisição de financiamento (suporte); investigação (igual); metodologia (igual); administração de projeto (igual); recursos (suporte); software (suporte); supervisão (igual); validação (igual); visualização (suporte); redação do rascunho original (suporte); revisão e edição do manuscrito (suporte). KS: conceituação (igual); curadoria de dados (igual); análise formal (igual); aquisição de financiamento (igual); investigação (igual); metodologia (igual); administração de projeto (igual); recursos (igual); software (igual); supervisão (igual); validação (igual); visualização (igual); redação do rascunho original (igual); revisão e edição do manuscrito (igual). TP: conceituação (igual); curadoria de dados (igual); análise formal (igual); aquisição de financiamento (igual); investigação (igual); metodologia (igual); administração de projeto (igual); recursos (igual); software (igual); supervisão (igual); validação (igual); visualização (igual); redação do rascunho original (igual); revisão e edição do manuscrito (igual). EK: conceituação (igual); curadoria de dados (igual); análise formal (suporte); aquisição de financiamento (igual); investigação (igual); metodologia (igual); administração de projeto (suporte); recursos (suporte); software (suporte); supervisão (igual); validação (igual); visualização (igual); redação do rascunho original (suporte); revisão e edição do manuscrito (igual). DM: conceituação (igual); curadoria de dados (igual); análise formal (igual); aquisição de financiamento (suporte); investigação (suporte); metodologia (igual); administração de projeto (suporte); recursos (suporte); software (suporte); supervisão (igual); validação (igual); visualização (igual); redação do rascunho original (igual); revisão e edição do manuscrito (igual). Todos os autores aprovaram a versão final do manuscrito.
CONFLITOS DE INTERESSE Nenhum declarado.
REFERÊNCIAS 1. World Health Organization. Europe [homepage on the Internet. Geneva: WHO; [cited 2022 Jul 21]. Coronavirus disease (COVID-19) pandemic. Available from: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019-ncov
2. National Institutes of Health. National Institute of Allergy and Infectious Diseases [homepage on the Internet]. Bethesda: NIAID; [cited 2022 Jul 21]. Coronaviruses. Available from: https://www.niaid.nih.gov/diseases-conditions/coronaviruses
3. YouGov-Cambridge Centre [homepage on the Internet]. London: YouGov; [cited 2022 Jul 21]. YouGov Cambridge Globalism 2020 Fieldwork Dates: 30th July - 24th August 2020. Available from: https://docs.cdn.yougov.com/msvke1lg9d/Globalism2020%20Guardian%20Conspiracy%20Theories.pdf
4. Zhong BL, Luo W, Li HM, Zhang QQ, Liu XG, Li WT, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745-1752. https://doi:10.7150/ijbs.45221
5. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes and practices towards COVID-19: A cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. https://doi:10.1371/journal.pone.0233668
6. Mahmood S, Hussain T, Mahmood F, Ahmad M, Majeed A, Beg BM, et al. Attitude, Perception, and Knowledge of COVID-19 Among General Public in Pakistan. Front Public Health. 2020;8:602434..https://doi:10.3389/fpubh.2020.602434
7. Siddiqui AA, Alshammary F, Amin J, Rathore HA, Hassan I, Ilyas M, et al. Knowledge and practice regarding prevention of COVID-19 among the Saudi Arabian population. Work. 2020;66(4):767-775.. https://doi:10.3233/WOR-203223
8. Alobuia WM, Dalva-Baird NP, Forrester JD, Bendavid E, Bhattacharya J, Kebebew E. Racial disparities in knowledge, attitudes and practices related to COVID-19 in the USA. J Public Health (Oxf). 2020;42(3):470-478. https://doi:10.1093/pubmed/fdaa069
9. Mubeen SM, Kamal S, Kamal S, Balkhi F. Knowledge and awareness regarding spread and prevention of COVID-19 among the young adults of Karachi. J Pak Med Assoc. 2020;70(Suppl 3)(5):S169-S174. https://doi:10.5455/JPMA.40
10. Xu H, Gonzalez Mendez MJ, Guo L, Chen Q, Zheng L, Chen P, et al. Knowledge, Awareness, and Attitudes Relating to the COVID-19 Pandemic Among Different Populations in Central China: Cross-Sectional Survey. J Med Internet Res. 2020;22(10):e22628. https://doi:10.2196/22628
11. Raftopoulos A, Theodosopoulou H. Scale validation methodology. Arch Hellenic Med. 2002;19(5):577–589.
12. Chen Y, Jin YL, Zhu LJ, Fang ZM, Wu N, Du MX, et al. The network investigation on knowledge, attitude and practice about Novel coronavirus pneumonia of the residents in Anhui Province [Article in Chinese]. Zhonghua Yu Fang Yi Xue Za Zhi. 2020;54(0):E004. https://doi:10.3760/cma.j.issn.0253-9624.2020.0004
13. González-Padilla DA, Tortolero-Blanco L. Social media influence in the COVID-19 Pandemic. Int Braz J Urol. 2020;46(suppl.1):120-124. https://doi:10.1590/S1677-5538.IBJU.2020.S121
14. Wakefield MA, Loken B, Hornik RC. Use of mass media campaigns to change health behaviour. Lancet. 2010;376(9748):1261-1271. https://doi:10.1016/S0140-6736(10)60809-4
15. Vasilopoulos A, Roupa Z, Gourgoulianis K. The influence of advertising messages on the smoking habits of teenagers. Pneumon. 2011;24(2):188-193.
16. Anastassea-Vlachou K, Fryssira-Kanioura H, Papathanasiou-Klontza D, Xipolita-Zachariadi A, Matsaniotis N. The effects of television viewing in Greece, and the role of the paediatrician: a familiar triangle revisited. Eur J Pediatr. 1996;155(12):1057-1060. https://doi:10.1007/BF02532531
17. Dkhar SA, Quansar R, Saleem SM, Khan SMS. Knowledge, attitude, and practices related to COVID-19 pandemic among social media users in J&K, India. Indian J Public Health. 2020;64(Supplement):S205-S210. https://doi:10.4103/ijph.IJPH_469_20
18. Yan Q, Tang Y, Yan D, Wang J, Yang L, Yang X, et al. Impact of media reports on the early spread of COVID-19 epidemic. J Theor Biol. 2020;502:110385. https://doi:10.1016/j.jtbi.2020.110385
19. Noar SM, Austin L. (Mis)communicating about COVID-19: Insights from Health and Crisis Communication. Health Commun. 2020;35(14):1735-1739. https://doi:10.1080/10410236.2020.1838093




 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket






