ABSTRACT
The objective of this study was to describe country-specific lockdown measures and tuberculosis indicators collected during the first year of the COVID-19 pandemic. Data on lockdown/social restrictions (compulsory face masks and hand hygiene; international and local travel restrictions; restrictions to family visits, and school closures) were collected from 24 countries spanning five continents. The majority of the countries implemented multiple lockdowns with partial or full reopening. There was an overall decrease in active tuberculosis, drug-resistant tuberculosis, and latent tuberculosis cases. Although national lockdowns were effective in containing COVID-19 cases, several indicators of tuberculosis were affected during the pandemic.
Keywords:
COVID-19; Tuberculosis; Physical distancing; Health policy; Global health; Communicable disease control.
RESUMO
O objetivo deste estudo foi descrever as medidas de confinamento específicas de cada país e os indicadores de tuberculose coletados durante o primeiro ano da pandemia de COVID-19. Dados referentes a confinamento/restrições sociais (uso obrigatório de máscaras faciais e higiene obrigatória das mãos; restrições a viagens internacionais e locais; restrições a visitas familiares e fechamento das escolas) foram coletados de 24 países em cinco continentes. A maioria dos países implantou múltiplos confinamentos, com reabertura parcial ou total. Houve uma redução geral dos casos de tuberculose ativa, tuberculose resistente e tuberculose latente. Embora os confinamentos nacionais tenham sido eficazes na contenção dos casos de COVID-19, vários indicadores de tuberculose foram afetados durante a pandemia.
Palavras-chave:
COVID-19; Tuberculose; Distanciamento físico; Política de Saúde; Saúde Global; Controle de doenças transmissíveis.
À medida que a pandemia de COVID-19 progredia, e em virtude da falta de vacinas ou tratamentos prontamente disponíveis, foram implantadas medidas de saúde pública destinadas a conter a disseminação da doença: diagnóstico rápido, isolamento rápido de casos, distanciamento físico, uso de máscaras faciais, fechamento de escolas, trabalho inteligente, restrições de viagens e fechamento de fronteiras internacionais. Países em todo o mundo implantaram confinamentos nacionais para conter a disseminação do vírus e reduzir o número de casos.(1) Por outro lado, estudos demonstraram que a pandemia de COVID-19 afetou substancialmente os serviços de tuberculose em muitos países.(2,3) Para avaliar as melhores práticas e as lições aprendidas, coletamos dados a respeito das medidas de confinamento adotadas por diversos países para administrar a pandemia. Nosso objetivo foi descrever essas medidas de confinamento específicas de cada país e os indicadores de controle da tuberculose coletados no mesmo período.
Convites para participar do estudo foram enviados a 24 países (aos coordenadores do estudo). Os dados foram coletados retrospectivamente desde o início das medidas de confinamento até 31 de dezembro de 2020. Foram coletados dados referentes a confinamento e outras restrições sociais (uso obrigatório de máscaras faciais e higiene obrigatória das mãos; restrições a viagens internacionais e locais; restrições a visitas familiares e fechamento das escolas), incluindo as datas e se as medidas foram implantadas total ou parcialmente. Também foram coletados os indicadores de controle da tuberculose (número total de casos de tuberculose, casos de tuberculose resistente, casos recém-diagnosticados de tuberculose e casos de tuberculose latente).
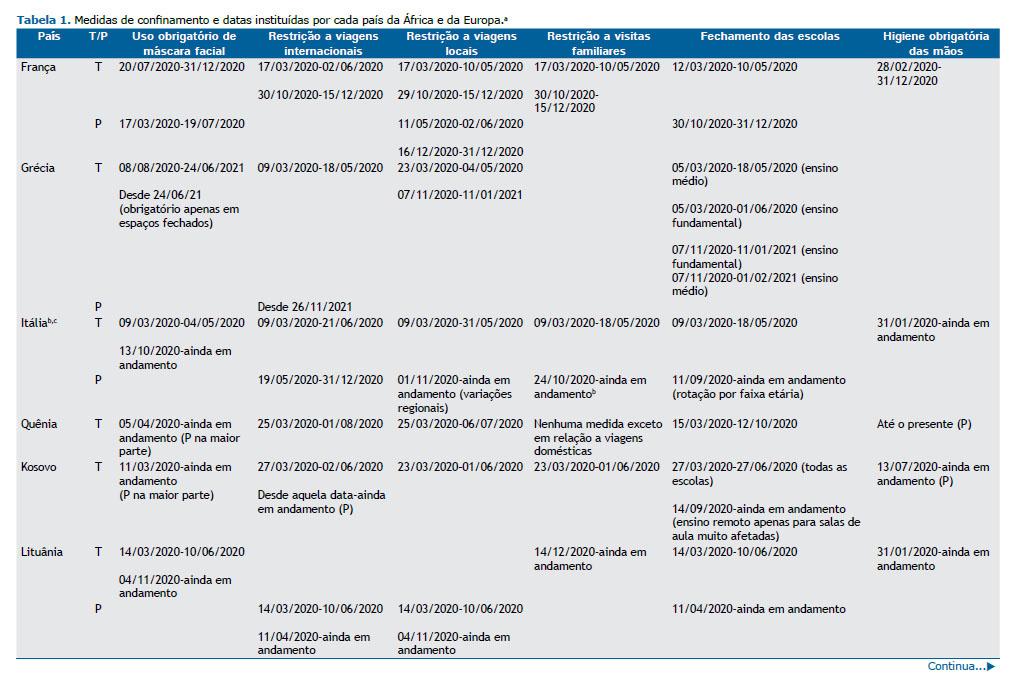
Foram coletados dados a respeito das medidas preventivas nacionais em 24 países de cinco continentes: 10 na Europa (França, Grécia, Itália, Kosovo, Lituânia, Países Baixos, Portugal, Rússia, Espanha e Reino Unido), 6 na Ásia (Butão, Camboja, Índia, Omã, Filipinas e Cingapura), 5 na América (Argentina, Brasil, México, Paraguai e EUA), 2 na África (Quênia e Níger) e 1 na Oceania (Austrália). As Tabelas 1 e 2 mostram esses dados, distribuídos por continente e país.
Medidas de confinamento foram implantadas em todos os países pesquisados. O primeiro confinamento foi na Austrália, em 1º de fevereiro de 2020, e o último foi em Cingapura, em 7 de abril de 2020. A maioria dos países implantou múltiplos confinamentos, com reabertura parcial ou total. O uso obrigatório de máscaras faciais foi parcial apenas no México e no Quênia. A higiene obrigatória das mãos foi implantada completamente em todos os países incluídos no estudo, exceto no Quênia, no qual foi implantada apenas parcialmente. As viagens internacionais foram parcialmente restringidas no Brasil, Camboja, Lituânia, Rússia, Cingapura, Reino Unido e EUA. As viagens locais foram parcialmente restringidas no Brasil, Camboja, Lituânia e Níger. Nos Países Baixos, nem viagens internacionais nem locais foram restringidas. No México, nenhuma medida foi tomada no que tange a viagens locais. As Filipinas não relataram restrições a viagens internacionais ou locais. Restrições a visitas familiares ocorreram na Austrália, Camboja, Países Baixos, Portugal, Rússia, Reino Unido e EUA. No Brasil, Quênia, México e Níger, nenhuma medida foi tomada no que tange a visitas familiares. O fechamento completo das escolas ocorreu em todos os países incluídos no estudo, exceto na Rússia, onde as escolas foram fechadas apenas parcialmente.
Os casos de tuberculose diminuíram de 32.898 em 2019 para 16.396 em 2020, com queda repentina em março de 2020 nos centros pesquisados, concomitantemente ao início dos confinamentos na maioria dos países. Essa diminuição foi observada em todos os países incluídos neste estudo, à exceção dos centros de tuberculose na Austrália, em Cingapura e no estado da Virgínia (EUA). O número de casos de tuberculose resistente também diminuiu (de 4.717 em 2019 para 1.527 em 2020), mesmo em países que têm um número menor de casos de tuberculose resistente, como a Argentina, o Brasil, a Índia, o México e a Rússia. Os casos de tuberculose recém-diagnosticada em ambulatórios diminuíram de 7.364 em 2019 para 5.703 em 2020, à exceção de centros na Austrália e no estado da Virgínia (EUA). Além disso, menos indivíduos receberam diagnóstico de tuberculose latente.
Vários fatores podem contribuir para explicar a relação entre pandemia de COVID-19/medidas de confinamento e indicadores de tuberculose. Para administrar a pandemia, recursos humanos e financeiros foram realocados dos serviços de tuberculose para as unidades de COVID-19, comprometendo a assistência à saúde de pacientes com tuberculose. Além disso, por medo de sair de casa (medo de infecção por SARS-CoV-2 ou medo do estigma), as pessoas evitaram ir a serviços de tuberculose e centros de saúde/hospitais em geral. O acesso aos serviços de tuberculose também foi dificultado em virtude das restrições de circulação e da redução do horário de funcionamento dos serviços de saúde. De fato, consultas e internações hospitalares em virtude de diversos quadros clínicos diminuíram drasticamente. As admissões ao departamento de emergência (DE) diminuíram mais de 50% em 2020 em comparação com 2019.(4) Os DE servem como linha de frente para pacientes com sintomas respiratórios em muitos países; muitos casos de tuberculose são diagnosticado em DE.(5) Em um estudo retrospectivo na Nigéria,(6) a tuberculose pulmonar foi diagnosticada em quase 30% dos adultos com queixas respiratórias em DE. Nesse sentido, a redução dos atendimentos em DE pode ter contribuído para a redução dos casos de tuberculose diagnosticados durante a pandemia.
Os testes de tuberculose e a terapia preventiva também foram impactados pela pandemia de COVID-19. Os testes de tuberculose diminuíram em alguns dos países incluídos no estudo, como as Filipinas, o Quênia e o Brasil. Foram descritas quedas relativas da terapia preventiva, de 30% a 70%, em diversos centros de tuberculose no Brasil, no Quênia, nas Filipinas e na Rússia, por exemplo.(2)
Observou-se uma queda do número de casos de tuberculose resistente notificados na Argentina, no Brasil, na Índia, no México e na Rússia. Globalmente, cerca de 45% menos pessoas realizaram o teste de tuberculose multirresistente (TBMR).(7) No Brasil, houve uma redução de 14% no consumo do teste Xpert MTB/RIF Ultra.(8) No entanto, a diminuição da taxa de consultas e do reconhecimento e detecção de doenças em virtude da pandemia podem resultar em atraso no diagnóstico e tratamento,(9) contribuindo para o aumento do número de casos de TBMR no futuro.
Para conter a disseminação do novo coronavirus, o público foi orientado a ficar em casa. No entanto, essa política pode não ser viável em alguns contextos. Nos países em desenvolvimento, os trabalhos informais são a maioria: 54% na América Latina, 67% no Sudeste Asiático e 86% na África.(10) Esses trabalhadores podem não ter a opção de ficar em casa, e nem todos os governos podem fornecer assistência financeira de emergência que os permita ficar em casa. Em alguns países da África (Egito, Quênia, Nigéria e África do Sul) e da América Latina (Peru, Brasil, Argentina, México e Colômbia), o tempo de deslocamento até o trabalho é significativamente afetado pelo nível de pobreza. Quanto mais elevado o nível de pobreza, menor a redução do tempo de deslocamento.(11) Nessas áreas de renda menor, o número de casos de COVID-19 pode ser maior e, consequentemente, pode haver menos recursos e conscientização voltados para outras doenças, tais como a tuberculose.
A adoção de medidas de permanência em casa e o uso de máscaras faciais em virtude da COVID-19 podem ter reduzido a transmissão de outras doenças transmissíveis, tais como a tuberculose. Por outro lado, políticas rígidas de contenção podem facilitar a disseminação domiciliar da tuberculose, já que o contato domiciliar é um dos fatores mais importantes na cadeia de transmissão da tuberculose.(12) No entanto, o impacto do aumento da transmissão domiciliar será percebido apenas nos próximos anos, pois a tuberculose tem um longo período de incubação.
Em centros de tuberculose na Austrália, em Cingapura e no estado da Virgínia (EUA), não se observou nenhuma redução do número de casos notificados de tuberculose. Esse achado pode ser atribuído ao aumento da vigilância tanto da tuberculose como da COVID-19 nesses locais. De fato, a adoção de mudanças organizacionais foi importante para a manutenção de consultas para problemas não relacionados à COVID-19. (9) Por exemplo, o Butão montou clínicas de gripe em todo o país para fazer a triagem de indivíduos com tosse e febre para reduzir o risco de transmissão da COVID-19. Aproveitando a infraestrutura e o investimento, o Butão também passou a realizar a triagem da tuberculose nas clínicas de gripe. Essa iniciativa apoiou os esforços de controle da tuberculose voltados para a busca ativa de casos e garantiu a continuidade dos serviços de tuberculose sem interrupção durante a pandemia de COVID-19. Além disso, é possível que o uso da telessaúde/telemedicina tenha evitado a redução dos diagnósticos de tuberculose.(9) Durante o confinamento, muitos locais implantaram a telessaúde; entretanto, ela infelizmente não está amplamente disponível em todos os centros de tuberculose.
Ainda não se sabe quais serão as futuras consequências da pandemia de COVID-19 e das medidas de confinamento. Cilloni et al.(13) estimaram que uma interrupção de três meses dos serviços de tuberculose causaria mais 1,19 milhões de casos de tuberculose e 361.000 mortes por tuberculose na Índia, além de 24.700 novos casos de tuberculose e 12.500 mortes por tuberculose no Quênia. O modelo da OMS sugere que os impactos negativos na mortalidade e incidência da tuberculose em 2020 tornar-se-ão muito piores nos próximos anos. Além disso, espera-se que a pandemia de COVID-19 tenha um impacto negativo nos determinantes da tuberculose, na renda média e nas taxas de desnutrição. Considerando que se pode atribuir 30-50% da incidência de tuberculose à desnutrição, o aumento da prevalência de desnutrição pode afetar a incidência e mortalidade da tuberculose. (7) Além disso, a Stop TB Partnership (Parceria para Acabar com a Tuberculose),(14) juntamente com outras instituições, realizou uma análise de modelagem para avaliar o impacto potencial da resposta à COVID-19 na tuberculose em países com alta carga da doença; os resultados sugerem que haverá mais 6,3 milhões de casos de tuberculose entre 2020 e 2025, além de mais 1,4 milhões de mortes por tuberculose no mesmo período.
Em suma, embora os confinamentos nacionais tenham sido eficazes na redução dos casos de COVID-19, vários indicadores de tuberculose foram drasticamente afetados durante a pandemia. Será preciso melhorar a vigilância, já que se pode esperar um aumento do número de casos de tuberculose, de casos de tuberculose resistente e de mortes por tuberculose nos próximos anos.
AGRADECIMENTOS Este artigo faz parte das atividades científicas da Global Tuberculosis Network, vinculada à World Association for Infectious Diseases and Immunological Disorders.
CONTRIBUIÇÕES DOS AUTORES DRS e GBM: redação do manuscrito. Todos os autores revisaram e aprovaram a versão final do manuscrito.
APROVAÇÃO ÉTICA O centro coordenador e os centros participantes receberam aprovação ética em conformidade com seus regulamentos institucionais.
CONFLITOS DE INTERESSES Nenhum conflito declarado.
REFERÊNCIAS 1. Abu-Raya B, Migliori GB, O’Ryan M, Edwards K, Torres A, Alffenaar JW, et al. Coronavirus Disease-19: An Interim Evidence Synthesis of the World Association for Infectious Diseases and Immunological Disorders (Waidid). Front Med (Lausanne). 2020;7:572485. https://doi.org/10.3389/fmed.2020.572485
2. Migliori GB, Thong PM, Alffenaar JW, Denholm J, Tadolini M, Alyaquobi F, et al. Gauging the impact of the COVID-19 pandemic on tuberculosis services: a global study. Eur Respir J. 2021;58(5):2101786. https://doi.org/10.1183/13993003.01786-2021
3. Migliori GB, Thong PM, Akkerman O, Alffenaar JW, Álvarez-Navascués F, Assao-Neino MM, et al. Worldwide Effects of Coronavirus Disease Pandemic on Tuberculosis Services, January-April 2020. Emerg Infect Dis. 2020;26(11):2709-2712. https://doi.org/10.3201/eid2611.203163
4. Mauro V, Lorenzo M, Paolo C, Sergio H. Treat all COVID 19-positive patients, but do not forget those negative with chronic diseases [published correction appears in Intern Emerg Med. 2021 Jan;16(1):249]. Intern Emerg Med. 2020;15(5):787-790. https://doi.org/10.1007/s11739-020-02395-z
5. Silva DR, Müller AM, Tomasini Kda S, Dalcin Pde T, Golub JE, Conde MB. Active case finding of tuberculosis (TB) in an emergency room in a region with high prevalence of TB in Brazil. PLoS One. 2014;9(9):e107576. https://doi.org/10.1371/journal.pone.0107576
6. Desalu OO, Ojo OO, Busari OA, Fadeyi A. Pattern of respiratory diseases seen among adults in an emergency room in a resource-poor nation health facility. Pan Afr Med J. 2011;9:24. https://doi.org/10.4314/pamj.v9i1.71199
7. World Health Organization [homepage on the Internet]. Geneva: WHO; c2022 [cited 2022 Jan 1]. Global Tuberculosis Report 2021. Available from: https://apps.who.int/iris/rest/bitstreams/1379788/retrieve
8. Brasil. Ministério da Saúde [homepage on the Internet]. Brasília: Ministério da Saúde [cited 2022 Jan 1]. Boletim Epidemiológico Tuberculose 2021. Available from: www.saude.gov.br.
9. Michalowsky B, Hoffmann W, Bohlken J, Kostev K. Effect of the COVID-19 lockdown on disease recognition and utilisation of healthcare services in the older population in Germany: a cross-sectional study. Age Ageing. 2021;50(2):317-325. https://doi.org/10.1093/ageing/afaa260
10. Pincombe M, Reese V, Dolan CB. The effectiveness of national-level containment and closure policies across income levels during the COVID-19 pandemic: an analysis of 113 countries. Health Policy Plan. 2021;36(7):1152-1162. https://doi.org/10.1093/heapol/czab054
11. Bargain O, Aminjonov U. Between a Rock and a Hard Place: Poverty and COVID-19 in Developing Countries. Institute of Labor Economics (IZA) [serial on the Internet] 2020 May [cited 2022 Jan 1]; IZA DP No. 13297 [23 p.]. Available from: https://www.iza.org/publications/dp/13297/between-a-rock-and-a-hard-place-poverty-and-covid-19-in-developing-countries https://doi.org/10.2139/ssrn.3614245
12. Acuña-Villaorduña C, Jones-López EC, Fregona G, Marques-Rodrigues P, Gaeddert M, Geadas C, et al. Intensity of exposure to pulmonary tuberculosis determines risk of tuberculosis infection and disease. Eur Respir J. 2018;51(1):1701578. https://doi.org/10.1183/13993003.01578-2017
13. Cilloni L, Fu H, Vesga JF, Dowdy D, Pretorius C, Ahmedov S, et al. The potential impact of the COVID-19 pandemic on the tuberculosis epidemic a modelling analysis. EClinicalMedicine. 2020;28:100603. https://doi.org/10.1016/j.eclinm.2020.100603
14. Stop TB Partnership [homepage on the Internet]. Geneva: WHO; c2022 [updated 2020 May 1; cited 2022 Jan 1]. The potential impact of the COVID-19 response on tuberculosis in high-burden countries: a modelling analysis. Available from: https://stoptb.org/assets/documents/news/Modeling%20Report_1%20May%202020_FINAL.pdf








 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket






