ABSTRACT
Objective: The objectives of this study were to determine reference values for sniff nasal inspiratory pressure (SNIP) and to propose reference equations for the population of Brazil. Methods: We evaluated 243 healthy individuals (111 males and 132 females), between 20 and 80 years of age, with an FVC and FEV1/FVC ratio > 80% and > 85% of the predicted value, respectively. All of the subjects underwent respiratory muscle strength tests to determine MIP, MEP, and SNIP. Results: We found that SNIP values were higher in males than in females (p < 0.05) and that SNIP correlated negatively with age, for males (r = −0.29; p < 0.001) and for females (r = −0.33; p < 0.0001). Linear regression also revealed that age influenced the predicted SNIP, for males (R2 = 0.09) and females (R2 = 0.10). We obtained predicted SNIP values that were higher than those obtained for other populations. Conclusions: We have devised predictive equations for SNIP to be used in adults (20-80 years of age) in Brazil. These equations could help minimize diagnostic discrepancies among individuals.
Keywords:
Respiratory Muscles; Respiratory Function Tests; Reference Values; Linear Models.
RESUMO
Objetivo: Os objetivos do presente estudo foram determinar equações de referência para pressão inspiratória nasal (PIN) e propor equações de referência para a população brasileira. Métodos: Foram avaliados 243 indivíduos saudáveis (111 homens e 132 mulheres), entre 20 e 80 anos, com CVF > 80% e razão VEF1/CVF > 85% do predito. Todos os indivíduos realizaram testes de força muscular respiratória para a determinação de PIN, PImáx e PEmáx. Resultados: Os valores da PIN foram maiores no sexo masculino que no feminino (p < 0,05), e a PIN apresentou correlação negativa com a idade para homens (r = −0,29; p < 0,001) e mulheres (r = −0,33; p < 0,0001). A análise de regressão linear múltipla também revelou que a idade permaneceu exercendo influência na predição da PIN em homens (R2 = 0,09) e mulheres (R2 = 0,10). Os valores preditos da PIN encontrados foram superiores àqueles obtidos em outras populações. Conclusões: Nesse contexto, sugerem-se equações preditivas para PIN em indivíduos brasileiros saudáveis na faixa etária entre 20 e 80 anos, com o intuito de minimizar discrepâncias diagnósticas ao comparar indivíduos.
Palavras-chave:
Músculos Respiratórios; Testes de Função Respiratória; Valores de Referência; Modelos Lineares.
IntroduçãoEm indivíduos com doença pulmonar, cardíaca ou neuromuscular, a disfunção dos musculus respiratórios é geralmente associada a complicações pulmonares, índices de morbidade elevados, qualidade de vida prejudicada e mortalidade.(1) A avaliação da musculatura respiratória é um método relevante para a detecção precoce dessa disfunção e para a quantificação desse declínio, fornecendo informações prognósticas e preditivas sobre a sobrevida desses pacientes.(1-3)
A determinação da pressão inspiratória nasal (PIN) é uma técnica volitiva não invasiva, facilmente aplicada, que é recomendada como um teste para complementar a avaliação da força muscular inspiratória (pela determinação da PImáx). A realização combinada de testes da musculatura inspiratória pode significativamente melhorar a acurácia de um diagnóstico de fraqueza da musculatura inspiratória.(4-6)
Valores normais de força muscular respiratória são úteis no estabelecimento, interpretação e diagnóstico da disfunção dos músculos respiratórios.(6,7) Dadas as características biológicas específicas de populações regionais, valores de referência devem ser obtidos para adultos saudáveis dos dois gêneros em uma dada região a fim de se evitar discrepâncias diagnósticas quando indivíduos ou populações são comparados.(8) Embora os valores preditivos de PIN foram estabelecidos para adultos brancos saudáveis,(6) adultos japoneses(9) e crianças brancas,(10) tais valores ainda não foram estabelecidos para adultos saudáveis no Brasil.
Os objetivos primários desse estudo foram determinar valores de referência de PIN para uma população de adultos saudáveis no Brasil, comparar valores de PIN máximos entre homens e mulheres e entre faixas etárias e propor equações de referência para a determinação de PIN no Brasil.
MétodosUm estudo transversal observacional multicêntrico foi realizado entre 2009 e 2011 em três centros de pesquisa. Os sujeitos foram estratificados em seis faixas etárias (20-29 anos, 30-39 anos, 40-49 anos, 50-59 anos, 60-69 anos e 70-80 anos). Como em estudos anteriores,(6,11) os sujeitos em cada faixa etária foram também divididos por gênero a fim de determinar valores de referência específicos para gênero. Os indivíduos foram avaliados em termos de dados sociodemográficos, hábitos de vida, doenças prévias ou atuais, parâmetros antropométricos (peso, altura e índice de massa corpórea [IMC]) e função pulmonar (por espirometria). Os participantes do estudo também foram avaliados quanto às pressões respiratórias (PImáx e PEmáx), PIN e padrão habitual de atividade física. Em cada centro de pesquisa, um único examinador realizou a avaliação em um único dia. O peso e a altura foram medidos com uma balança antropométrica (Filizola®, São Paulo, Brasil). Determinamos o IMC com a seguinte fórmula: IMC = peso/altura2 (kg/m2).(12)
A amostra foi composta por indivíduos das cidades de Natal (RN), Recife (PE) e Piracicaba (SP). Os critérios de inclusão foram ser saudável, não ser um atleta, ter entre 20 e 80 anos de idade,(6) ter IMC entre 18,5 e 29,9 kg/m2 e ser não fumante.(8) Sujeitos com história de doença respiratória (asma, bronquite crônica, tuberculose, DPOC ou enfisema) foram excluídos, assim como aqueles com história de doença neuromuscular, cerebrovascular ou cardíaca (infarto do miocárdio ou insuficiência cardíaca)(8,13,14); aqueles com rinite, sinusite ou desvio de septo; os que haviam sido submetidos à cirurgia nasal; os com gripe ou resfriado na semana anterior à avaliação(11); os em uso regular de medicação para alergias respiratórias; os em uso de corticosteroides orais, depressores do sistema nervoso central, barbitúricos ou relaxantes musculares(14,15); as grávidas(9); os com CVF 80% do previsto; e os com relação VEF1/CVF 85% do previsto.(6) Indivíduos incapazes de entender ou realizar as manobras exigidas para a avaliação também foram excluídos do estudo. Nenhum dos participantes havia sido exposto a técnicas de medição da força muscular respiratória. O estudo foi aprovado pelo Comitê de Ética em Pesquisa do Hospital Universitário (Protocolo no. 260/08), e todos os sujeitos assinaram o termo de consentimento livre e esclarecido. Todos os procedimentos foram realizados de acordo com os padrões éticos estabelecidos na Declaração de Helsinki.(16)
A espirométrica foi realizada com um espirômetro DATOSPIR-120C® (Sibelmed, Barcelona, Espanha), adequadamente calibrado, e todos os testes espirométricos foram realizados de acordo com as diretrizes da American Thoracic Society/European Respiratory Society (ATS/ERS).(17) Foram determinados CVF, VEF1 e relação VEF1/CVF. Os resultados (obtidos em valores absolutos e relativos) foram comparados com valores de referência previamente publicados.(18)
A força muscular respiratória foi avaliada com base nas pressões respiratórias máximas (PImáx e PEmáx). Após receberem instruções quanto ao procedimento, os sujeitos foram avaliados com um manômetro digital MicroRPM® (Micro Medical, Rochester, Reino Unido), e os testes foram realizados de acordo com as normas e recomendações da ATS/ERS.(4) Os resultados foram obtidos em valores absolutos e comparados com valores de referência anteriormente publicados.(11) A PImáx foi medida com um bocal cilíndrico descartável conectado ao manômetro. Os sujeitos realizaram uma manobra de inspiração máxima a partir do VR. Na determinação da PEmáx, os sujeitos realizaram uma manobra de expiração máxima a partir da CPT.
Na avaliação de PIN, o sujeito permanecia sentado, com uma narina ocluída por um plug nasal de silicone conectado ao manômetro digital MicroRPM® por um cateter de polietileno (diâmetro interno, 1 mm). Medimos a PIN a partir da capacidade residual funcional (CRF). Os sujeitos, com a boca fechada, realizavam uma manobra de inspiração máxima através da narina contralateral patente ao final de uma expiração normal e lenta.(4,6,11) Dez manobras foram executadas.(6,19) Os critérios utilizados na seleção das inspirações mais bem tecnicamente aceitáveis incluíram uma manobra com uma pressão de pico mantida por ao menos 0,5 s e um período de descanso entre as manobras de 30 s. O programa Puma (The University of Manchester, Manchester, Reino Unido) foi utilizado; esse programa identifica automaticamente as manobras aceitáveis e as armazena em um banco de dados. Não houve feedback visual durante as manobras,e o maior valor obtido foi utilizado na análise dos dados.
Foi administrada a versão em português do Brasil do questionário Baecke para a medida de atividade física habitual (AFH), que fora adaptado culturalmente e validado para uso no Brasil.(20) O questionário avalia as percepções individuais sobre as atividades físicas durante o tempo de lazer, assim como o lazer e a locomoção nos últimos 12 meses. As respostas são pontuadas em uma escala de 0 a 5 pontos, e o resultado final é expresso em um índice resumido.
O tamanho da amostra foi calculado utilizando-se um teste t baseado na população media e desvio-padrão máximo de PIN determinado no estudo de Uldry Fitting,(6) e valores de p < 0,05 (poder de 99% com intervalo de confiança de 5%) foram considerados estatisticamente significantes. O tamanho da amostra sugerido foi de 260 indivíduos, com um coeficiente de correlação interclasse esperado de 7,86 cmH2O. Os dados foram expressos como média ± dp. O teste de Kolmogorov-Smirnov foi aplicado para a determinação da normalidade da distribuição dos dados. Foram comparados os valores de PImáx, PEmáx e PIN entre os gêneros com testes t não pareados e entre faixas etárias com ANOVA. Se uma razão F significativa era obtida, comparações pós-teste eram realizadas com o teste de Newman-Keuls. O coeficiente de correlação de Pearson foi aplicado a fim de correlacionar PIN com as variáveis do estudo. A análise de regressão linear foi utilizada para se obter equações preditivas para as variáveis independentes que se correlacionaram com PIN. Os limites inferiores do modelo de regressão foram calculados do quinto percentil do desvio-padrão residual, assumindo-se uma distribuição gaussiana, e foram estimados da seguinte forma(21):
limite inferior = valor previsto − 1,645 × EPE
onde EPE é o erro-padrão estimado.
A probabilidade de um erro tipo I erro adotada foi de 0,05 para todos os testes. As análises estatísticas foram realizadas com o programa Statistical Package for the Social Sciences, versão 15 (SPSS Inc., Chicago, IL, EUA).
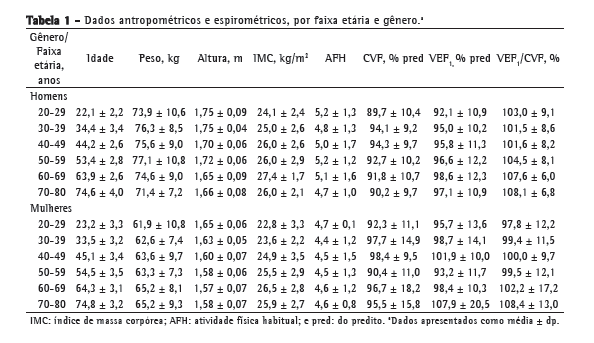
ResultadosOs voluntários foram recrutados na comunidade e avaliados em uma entrevista preliminar, como pode ser visto na Figura 1. As características demográficas e de estilo de vida, assim como os parâmetros antropométricos e os dados espirométricos, estão detalhados na Tabela 1.

Os valores de pressão respiratória estão apresentados na Tabela 2. De forma geral, os valores médios de PImáx, PEmáx e PIN foram significantemente maiores em homens do que em mulheres (114,3 ± 28,6 cmH2O vs. 92,6 ± 19,7 cmH2O; p < 0,05). Em cada gênero, foram também encontradas diferenças significantes entre as faixas etárias (p < 0,05), como mostrado na Tabela 2. As correlações entre PIN e as variáveis estudadas estão apresentadas na Tabela 3. Houve correlação negativa entre PIN e idade tanto para homens (r = −0,29; p < 0,001) como para mulheres (r = −0,33; p < 0,0001). Entretanto, a PIN não se correlacionou significantemente com o peso, altura, IMC ou AFH nos dois gêneros. Após a regressão linear, a única variável que manteve a significância foi a idade, que se mostrou preditora da PIN para homens (p < 0,001) e mulheres (p < 0,0001) e, portanto, foi incluída no modelo das equações preditivas de PIN em função da idade (Tabela 4):



Homens: PIN = 135,6 − 0,47 ×
(idade) (R2 = 0,09; EPE = 27,4)
Mulheres: PIN = 110,1 − 0,36 ×
(idade) (R2 = 0,10; EPE = 18,6)
onde R2 é o coeficiente da determinação. As médias dos limites inferiores são calculados pela subtração de 1,645 vezes o desvio-padrão residual da média.
DiscussãoOs objetivos do presente estudo foram determinar valores de referência para PIN em uma população de adultos saudáveis no Brasil; comparar os valores máximos de PIN entre homens e mulheres, assim como entre as faixas etárias; e propor equações de referência para PIN para brasileiros. Nossos resultados mostram que a idade tem uma influência negativa na PIN e é também preditora da PIN, podendo, portanto, ser incluída em equações de regressão linear para a determinação de valores de referência.
Vários estudos mencionaram a importância da PIN como um teste da força dos músculos respiratórios que é válido, não invasivo e fácil de ser aplicado, podendo ser utilizado como um complemento à PImáx.(5,6) Este é o terceiro estudo na literatura a propor valores de referência para PIN em adultos saudáveis e o primeiro para a população brasileira. Os resultados do presente estudo mostram que a PIN foi significantemente menor nas mulheres que nos homes, e isso provavelmente é devido à maior massa muscular dos homens, o que corrobora os achados de outros estudos sobre a força muscular respiratória.(11,21,22) Em termos de valores de PIN, houve diferenças significantes entre as faixas etárias (em cada gênero) e uma queda com a idade. Isso pode ser atribuído à redução da força muscular inspiratória durante o processo de envelhecimento, resultante da sarcopenia; à perda de massa muscular(22-24); e à perda de viscoelasticidade dos pulmões e da caixa torácica,(23) associados ao aumento da gordura abdominal, que pode interferir com a biomecânica do diafragma.(11) Entre as variáveis independentes (idade, peso, altura, IMC e AFH), somente a idade foi correlacionada com a PIN (correlação negativa fraca), o que está de acordo com os achados de Uldry Fitting(6) e, somente para homens, com aqueles de Kamide et al.(9) Uldry Fitting(6) também relataram que o peso e o IMC não se correlacionaram com a PIN. Embora a força muscular respiratória esteja diretamente relacionada ao nível de atividade física,(11) AFH não teve correlação com a PIN em homens ou mulheres. Devemos lembrar que o questionário de Baecke somente fornece um índice, sem caracterizar o nível de atividade física, o que dificulta a identificação do estilo de vida sedentário.(25) Os valores de referência de PIN obtidos no presente estudo diferiram daqueles relatados para homens e mulheres jovens no Japão (76,8 ± 28,9 cmH2O e 60 ± 20 cmH2O, respectivamente). Nossa análise de regressão linear demonstrou que as equações preditivas decorreram da PIN em função da idade para ambos os gêneros, o que corrobora os achados de Uldry Fitting(6) e de Kamide et al.,(9) exceto pelo fato de que Kamide et al. relataram que a PIN somente se correlacionou com o IMC no caso das mulheres. Isso contrasta com relatos da influência negativa da idade sobre a força muscular respiratória,(21-23) assim como da relação entre a massa muscular respiratória e a massa magra, que é mais evidente em homens.(11,21) Um aspecto importante dos nossos resultados é que o coeficiente de determinação para a idade no modelo de regressão linear foi baixo em homens e mulheres (R2 = 0,09 e R2 = 0,1, respectivamente), embora esse achado seja análogo aos de Uldry Fitting (R2 = 0,09 e R2 = 0,05, respectivamente) e de Kamide et al. (R2 = 0,14 para homens).(6,9) De acordo com a ATS,(21) a ampla variabilidade em valores de referência é devida a diferenças metodológicas que podem influenciar a avaliação da função pulmonar, incluindo a técnica de medição e os aspectos individuais, biológicos e populacionais. Nesse contexto, devemos destacar algumas diferenças entre o presente estudo e aqueles conduzidos por Uldry Fitting(6) e Kamide et al.(9) A nossa investigação seguiu as recomendações da ATS(21) e foi baseada em metodologias de estudos anteriores para a obtenção de equações de referência para função pulmonar(14,18) e muscular.(6,11,19) Outro fator a ser considerado é que pode haver diferenças étnicas e individuais em uma dada população. Em comparação com populações em países europeus e do Japão, a população brasileira é etnicamente heterogênea. Os valores de referência devem ser baseados em dados recentes, e as equações preditivas para PIN mais recentes foram publicadas em 1995 e 2009.(6,9) Mudanças sociodemográficas e ambientais provavelmente influenciam os resultados e, portanto, tais dados devem ser periodicamente atualizados. Dessa forma, as diferenças observadas podem ser atribuídas a diferenças na avaliação técnica, no equipamento e nas características da população.
Embora o presente estudo demonstre poder, certas limitações devem ser observadas. Primeiro, os valores de PIN foram baseados na CRF sem monitorização. Entretanto, essa foi considerada como sendo ao final de uma expiração normal, já relatada em outros estudos, e a determinação da CRF tornaria a técnica de PIN cara e inacessível. Outra limitação potencial foi a não inclusão de indivíduos com mais de 80 anos de idade e, consequentemente, as equações preditivas propostas não seriam válidas para indivíduos acima dessa idade.
Com base nos valores médios obtidos em nossa amostra, foram criadas equações preditivas para PIN para a população brasileira. Essas equações podem ser usadas na avaliação diagnóstica de brasileiros entre 20 e 80 anos de idade.
AgradecimentosAgradecemos a todos os participantes, cujas contribuições tornaram possível o presente estudo.
Referências1. Iandelli I, Gorini M, Misuri G, Gigliotti F, Rosi E, Duranti R, et al. Assessing inspiratory muscle strength in patients with neurologic and neuromuscular diseases: comparative evaluation of two noninvasive techniques. Chest. 2001;119(4):1108-13. PMid:11296177. http://dx.doi.org/10.1378/chest.119.4.1108
2. Rocha JA, Miranda MJ. Ventilatory dysfunction in motor neuron disease: when and how to act? [Article in Portuguese]. Acta Med Port. 2007;20(2):157-65. PMid:17868522.
3. Morgan RK, McNally S, Alexander M, Conroy R, Hardiman O, Costello RW. Use of Sniff nasal-inspiratory force to predict survival in amyotrophic lateral sclerosis. Am J Respir Crit Care Med. 2005;171(3):269-74. PMid:15516537. http://dx.doi.org/10.1164/rccm.200403-314OC
4. American Thoracic Society/European Respiratory Society. ATS/ERS Statement on respiratory muscle testing. Am J Respir Crit Care Med. 2002;166(4):518-624. PMid:12186831. http://dx.doi.org/10.1164/rccm.166.4.518
5. Steier J, Kaul S, Seymour J, Jolley C, Rafferty G, Man W, et al. The value of multiple tests of respiratory muscle strength. Thorax. 2007;62(11):975-80. PMid:17557772 PMCid:2117126. http://dx.doi.org/10.1136/thx.2006.072884
6. Uldry C, Fitting JW. Maximal values of sniff nasal inspiratory pressure in healthy subjects. Thorax. 1995;50(4):371-5. http://dx.doi.org/10.1136/thx.50.4.371
7. Hughes PD, Polkey MI, Kyroussis D, Hamnegard CH, Moxham J, Green M. Measurement of sniff nasal and diaphragm twitch mouth pressure in patients. Thorax. 1998;53(2):96-100. PMid:9624292 PMCid:1758721. http://dx.doi.org/10.1136/thx.53.2.96
8. Sociedade Brasileira de Pneumologia e Tisiologia. Diretrizes para testes de função pulmonar. J Pneumol. 2002;28(3):S1-238.
9. Kamide N, Ogino M, Yamashina N, Fukuda M. Sniff nasal inspiratory pressure in healthy Japanese subjects: mean values and lower limits of normal. Respiration. 2009;77(1):58-62. PMid:18957838. http://dx.doi.org/10.1159/000167321
10. Stefanutti D, Fitting JW. Sniff nasal inspiratory pressure. Reference values in Caucasian children. Am J Respir Crit Care Med. 1999;159(1):107-11. PMid:9872826.
11. Neder JA, Andreoni S, Lerario MC, Nery LE. Reference values for lung function tests. II. Maximal respiratory pressures and voluntary ventilation. Braz J Med Biol Res. 1999;32(6):719-27. PMid:10412550. http://dx.doi.org/10.1590/S0100-879X1999000600007
12. Coutinho W. Consenso latino-americano de obesidade. Arq Bras Endocrinol Metab.1999;43(1):21-67. http://dx.doi.org/10.1590/S0004-27301999000100003
13. Souza RB. Pressões respiratórias estáticas máximas. J Pneumol. 2002;28(Suppl 3):S155-S165.
14. Neder JA, Andreoni S, Castelo-Filho A, Nery LE. Reference values for lung function tests. I. Static volumes. Braz J Med Biol Res. 1999;32(6):703-17. PMid:10412549. http://dx.doi.org/10.1590/S0100-879X1999000600006
15. Harik-Khan RI, Wise RA, Fozard JL. Determinants of maximal inspiratory pressure. The Baltimore Longitudinal Study of Aging. Am J Respir Crit Care Med. 1998;158(5 Pt 1):1459-64. PMid:9817693.
16. World Medical Association - WMA [homepage on the Internet]. Ferney-Voltaire: World Medical Association [cited 2011 Jun 26]. WMA Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects. Available from: http://www.wma.net/en/30publications/10policies/b3/
17. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319-38. PMid:16055882. http://dx.doi.org/10.1183/09031936.05.00034805
18. Pereira CA, Sato T, Rodrigues SC. New reference values for forced spirometry in white adults in Brazil. J Bras Pneumol. 2007;33(4):397-406. PMid:17982531. http://dx.doi.org/10.1590/S1806-37132007000400008
19. Lofaso F, Nicot F, Lejaille M, Falaize L, Louis A, Clement A, et al. Sniff nasal inspiratory pressure: what is the optimal number of sniffs? Eur Respir J. 2006;27(5):980-2. PMid:16455823.
20. Florindo AA, Latorre MR. Validação e reprodutibilidade do questionário de Baecke de avaliação da atividade física habitual em homens adultos. Rev Bras Med Esporte. 2003;9(3):121-8.
21. Lung function testing: selection of reference values and interpretative strategies. American Thoracic Society. Am Rev Respir Dis. 1991;144(5):1202-18. PMid:1952453. http://dx.doi.org/10.1164/ajrccm/144.5.1202
22. Simões RP, Deus AP, Auad MA, Dionísio J, Mazzonetto M, Borghi-Silva A. Maximal respiratory pressure in healthy 20 to 89 year-old sedentary individuals of central São Paulo State. Rev Bras Fisioter. 2010;14(1):60-7. PMid:20414563. http://dx.doi.org/10.1590/S1413-35552010000100010
23. Enright PL, Kronmal RA, Manolio TA, Schenker MB, Hyatt RE. Respiratory muscle strength in the elderly. Correlates and reference values. Cardiovascular Health Study Research Group. Am J Respir Crit Care Med. 1994;149(2 Pt 1):430-8. PMid:8306041.
24. Pride NB. Ageing and changes in lung mechanics. Eur Respir J. 2005;26(4):563-5. PMid:16204583. http://dx.doi.org/10.1183/09031936.05.00079805
25. Simões LA, Dias JM, Marinho KC, Pinto CL, Britto RR. Relationship between functional capacity assessed by walking test and respiratory and lower limb muscle function in community-dwelling elders [Article in Portuguese]. Rev Bras Fisioter. 2010;14(1):24-30. PMid:20414558. http://dx.doi.org/10.1590/S1413-35552010000100005
* Trabalho realizado na Universidade Federal do Rio Grande do Norte - UFRN - Natal (RN) Brasil; na Universidade Federal do Pernambuco - UFPE - Recife (PE) Brasil; e na Universidade Metodista de Piracicaba - UNIMEP - Piracicaba (SP) Brasil.
Endereço para correspondência: Guilherme Augusto de Freitas Fregonezi. Laboratório de Desempenho Pneumocardiovascular e Músculos Respiratórios, Universidade Federal do Rio Grande do Norte, Caixa Postal 1524, Campus Universitário Lagoa Nova, CEP 59072-970, Natal, RN, Brasil.
Tel. 55 84 3342-2001. E-mail: fregonezi@ufrnet.br
Apoio financeiro: Vanessa Regiane Resqueti é bolsista de Desenvolvimento Científico Regional (DCR) do Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq; Processo nº 0016-4.08/11). Guilherme Augusto de Freitas Fregonezi é bolsista de produtividade em pesquisa do CNPq - nível 2 (PQ-2; Processo nº 301661/2009-0).
Recebido para publicação em 15/5/2012. Aprovado, após revisão, em 18/9/2012.
Sobre os autores
Palomma Russelly Saldanha Araújo
Doutoranda em Biotecnologia. Rede Nordeste de Biotecnologia - RENORBIO - Fortaleza (CE) Brasil; Fisioterapeuta da Secretaria de Saúde do Estado da Paraíba, João Pessoa (PB) Brasil.
Vanessa Regiane Resqueti
Professora de Fisioterapia. Laboratório de Terapia Respiratória, Departamento de Fisioterapia, Universidade Federal do Pernambuco - UFPE - Recife (PE) Brasil.
Jasiel Nascimento Jr
Fisioterapeuta. Universidade Federal do Pernambuco - UFPE - Recife (PE) Brasil.
Larissa de Andrade Carvalho
Mestranda em Fisioterapia. Universidade Federal do Pernambuco - UFPE - Recife (PE) Brasil.
Ana Gabriela Leal Cavalcanti
Fisioterapeuta. Universidade Federal do Pernambuco - UFPE - Recife (PE) Brasil.
Viviane Cerezer Silva
Fisioterapeuta. Universidade Metodista de Piracicaba - UNIMEP - Piracicaba (SP) Brasil.
Ester Silva
Professora de Fisioterapia. Universidade Metodista de Piracicaba - UNIMEP - Piracicaba (SP) Brasil.
Marlene Aparecida Moreno
Professora de Fisioterapia. Universidade Metodista de Piracicaba - UNIMEP - Piracicaba (SP) Brasil.
Arméle de Fátima Dornelas de Andrade
Professora de Fisioterapia. Universidade Federal do Pernambuco - UFPE - Centro de Ciências da Saúde, Departamento de Fisioterapia. Laboratório de Fisioterapia Respiratória, Recife (PE) Brasil.
Guilherme Augusto de Freitas Fregonezi
Professor de Fisioterapia. Universidade Federal do Rio Grande do Norte - UFRN - Laboratório de Desempenho Pneumocardiovascular e Músculos Respiratórios, Departamento de Fisioterapia, Natal (RN) Brasil.











 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket