INTRODUCTION Pulmonary arterial hypertension (PAH) is a rare disease associated with high mortality due to right ventricular dysfunction. During PAH diagnostic workup, pulmonary function tests (PFTs) are essential to exclude relevant parenchymal lung disease. PFTs additionally provide information on PAH severity and prognosis.
OVERVIEW A 22-year-old woman reported a five-year history of progressive dyspnea, functional class II. After a detailed diagnostic workup, an idiopathic PAH (IPAH) diagnosis was made, and bosentan was started. Baseline PFT revealed an obstructive ventilatory pattern with normal lung volumes and a decreased DLCO (Panel 1A-C). She had never smoked and had no previous asthma diagnosis. During follow-up, the patient was treated with add-on triple therapy and was listed for lung transplantation. Eleven years after the onset of the disease, enlarged pulmonary arteries were evident by chest imaging. PFT showed a decrease in FVC, FEV1, and FEV1/FVC, with signs of air trapping and reduced DLCO and KCO (Panel 1D-F). In patients with PAH, a decreased DLCO is expected; however, without lung volume abnormalities. Additionally, DLCO is a marker of disease severity,(1-3) and a DLCO < 45% is related to aging, smoking history, lower exercise capacity, and worse survival on PAH. (3) KCO adds information to PFT interpretation, and low levels associated with normal VA are suggestive of pulmonary vascular disease or intrapulmonary right-to-left shunting, signaling inefficient gas exchange.(4) Both restrictive and obstructive PFT patterns have been described in PAH patients. It has been demonstrated that the worsening of lung function is related to PAH severity.(1-3) Notably, obstructive disturbance among PAH patients is more frequently found in congenital heart disease and connective tissue disease.(3) A recent study has demonstrated that patients with IPAH without lung disease have a better five-year-survival compared with those with mild lung disease (70% vs. 22%, respectively; p < 0.0001). However, the mechanisms underlying lung function disturbances in PAH remain unclear. The hypotheses of airflow obstruction are speculative, as an inflammatory response could have similar effects on vascular and airway smooth musculature, causing a proliferation in small airway wall thickening. Another possible explanation includes “competition for space” between hypertrophied vessels and distal airways within the interstitial space.(1,2) Recently, Rahaghi et al. analyzed PFT at baseline and at the time of lung transplantation in PAH and found a reduction in FEV1, FVC, and FEV1/FVC over time. There was no evidence of parenchymal or airway disorder in the pathology. Airflow obstruction correlated best with an expanded thoracic blood volume and increased pulmonary artery diameter despite unchanged pulmonary hemodynamics. In this context, airway compression secondary to pulmonary arteries dilatation may be a potential mechanism of peripheral airway obstruction in PAH. (4) Regarding DLCO, the reduction could be explained by increased alveolar-capillary membrane thickness related to endothelial cell proliferation and reduced perfused pulmonary capillary bed. However, the loss of alveolar-capillary membrane diffusing capacity and lung capillary blood volume could also explain a reduced DLCO in PAH.(1,2,5)
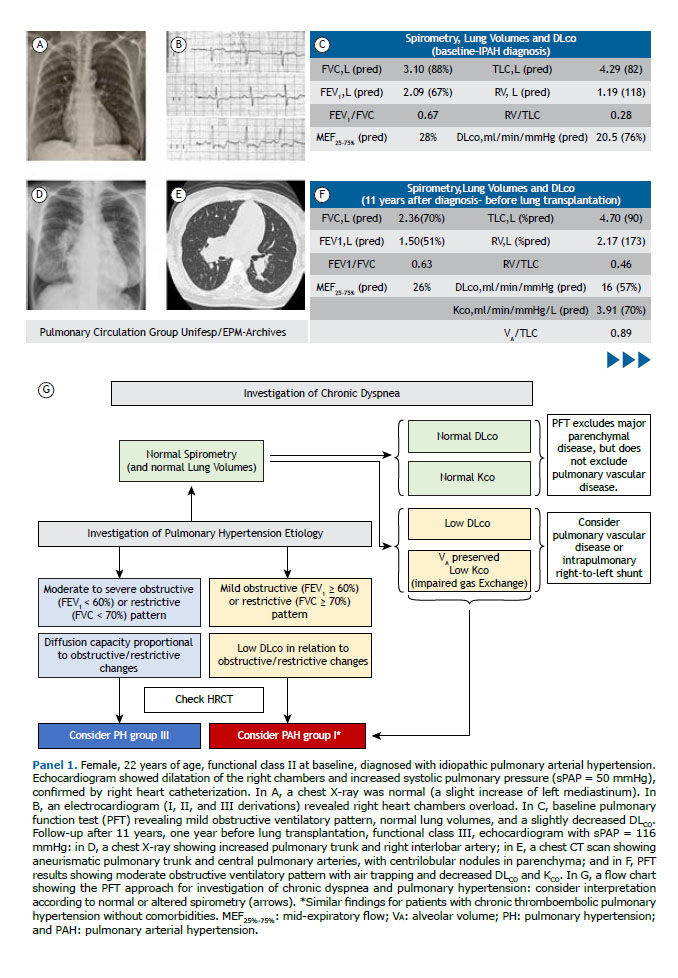
PFTs provide valuable information to monitor disease severity and prognosis in PAH. There is a continued interest in understanding the pathophysiology of lung function disturbances in PAH, aiming to improve PAH phenotyping and the potential impact on new targeted treatment approaches. An approach for PFT interpretation in the scope of chronic dyspnea and the investigation of PH etiology is described (Panel 1G).
AUTHOR CONTRIBUTIONS EVMF: elaboration, writing, and review. JSL: elaboration and writing. RKFO: review. All authors read and approved the final version of the manuscript.
CONFLICTS OF INTEREST None declared.
REFERENCES 1. Sun XG, Hansen JE, Oudiz RJ, Wasserman K. Pulmonary function in primary pulmonary hypertension. J Am Coll Cardiol. 2003;41(6):1028-1035. https://doi.org/10.1016/s0735-1097(02)02964-9
2. Jing ZC, Xu XQ, Badesch DB, Jiang X, Wu Y, Liu JM, et al. Pulmonary function testing in patients with pulmonary arterial hypertension. Respir Med. 2009;103(8):1136-1142. https://doi.org/10.1016/j.rmed.2009.03.009
3. Lewis RA, Thompson AAR, Billings CG, Charalampopoulos A, Elliot CA, Hamilton N, et al. Mild parenchymal lung disease and/or low diffusion capacity impacts survival and treatment response in patients diagnosed with idiopathic pulmonary arterial hypertension. Eur Respir J. 2020;55(6):2000041. https://doi.org/10.1183/13993003.00041-2020
4. Neder JA, Berton DC, Muller PT, O‘Donnell DE. Incorporating Lung Diffusing Capacity for Carbon Monoxide in Clinical Decision Making in Chest Medicine. Clin Chest Med. 2019;40(2):285-305. https://doi.org/10.1016/j.ccm.2019.02.005
5. Rahaghi FN, Trieu M, Shaikh F, Abtin F, Diaz AA, Liang LL, et al. Evolution of Obstructi-ve Lung Function in Advanced Pulmonary Arterial Hypertension. Am J Respir Crit Care Med. 2021;204(12):1478-1481. https://doi.org/10.1164/rccm.202105-1169LE




 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket






