ABSTRACT
Smoking is the leading cause of respiratory disease (RD). The harmful effects of smoking on the respiratory system begin in utero and influence immune responses throughout childhood and adult life. In comparison with "healthy" smokers, smokers with RD have peculiarities that can impede smoking cessation, such as a higher level of nicotine dependence; nicotine withdrawal; higher levels of exhaled carbon monoxide; low motivation and low self-efficacy; greater concern about weight gain; and a high prevalence of anxiety and depression. In addition, they require more intensive, prolonged treatment. It is always necessary to educate such individuals about the fact that quitting smoking is the only measure that will reduce the progression of RD and improve their quality of life, regardless of the duration and severity of the disease. Physicians should always offer smoking cessation treatment. Outpatient or inpatient smoking cessation treatment should be multidisciplinary, based on behavioral interventions and pharmacotherapy. It will thus be more effective and cost-effective, doubling the chances of success.
Keywords:
Respiratory tract diseases/therapy; Respiratory tract diseases/drug therapy; Tobacco use disorder/epidemiology; Smoking cessation; Counseling; Lung neoplasms.
RESUMO
O tabagismo é o maior responsável pelas doenças respiratórias (DR). Os efeitos nocivos do tabaco sobre o aparelho respiratório se iniciam ainda intraútero e influenciam as respostas imunológicas ao longo da infância e vida adulta. Os tabagistas com DR possuem peculiaridades que podem dificultar a cessação tabágica, tais como maior grau de dependência e de abstinência de nicotina; níveis mais elevados de monóxido de carbono exalado; motivação e autoeficácia baixas; maior preocupação com ganho ponderal; e elevada prevalência de ansiedade e depressão. Além disso, requerem tratamento mais intensivo e prolongado. É necessário esclarecer sempre o paciente sobre o fato de que parar de fumar será a única medida que irá reduzir a progressão das DR e melhorar sua qualidade de vida, independentemente do tempo e da gravidade da doença. Os médicos devem sempre oferecer o tratamento de cessação tabágica. O tratamento ambulatorial ou hospitalar deve ser multidisciplinar, baseado em intervenções comportamentais e farmacoterapia, sendo eficaz e custo-efetivo, dobrando as chances de sucesso.
Palavras-chave:
Doenças respiratórias/terapia; Doenças respiratórias/tratamento farmacológico; Tabagismo/epidemiologia, Abandono do uso do tabaco; Aconselhamento; Neoplasias pulmonares.
INTRODUÇÃOO tabagismo é a principal causa de morte evitável no mundo e é responsável por 7 milhões de óbitos anuais, 890 mil desses associados ao tabagismo passivo.(1) No Brasil, morrem 156 mil pessoas por ano por doenças relacionadas ao tabaco.(2) No mundo, há cerca de 1,1 bilhões de tabagistas que vivem, em sua maioria, em países de baixa e média renda, onde a carga da doença e mortalidade por tabaco é maior.(1)
A prevalência do tabagismo no Brasil tem caído de forma notável, conforme demonstra a série histórica de 2006-2017 da pesquisa "Vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico" (Vigitel), com redução de 48,2% (de 19,5% para 10,1%).(3) Em 2017, a pesquisa Vigitel revelou 10,1% de tabagistas (13,2% nos homens e 7,5% nas mulheres) no país, o que ainda representa 18,2 milhões de fumantes com idade acima de 18 anos.(3,4)
A Convenção-Quadro para o Controle do Tabaco(5) inclui a oferta para o tratamento da dependência nicotínica como uma das seis políticas mais custo-efetivas do pacote MPOWER, um acrônimo que significa Monitoring tobacco use (monitorar o uso do tabaco); Protecting people from tobacco smoke (proteger as pessoas da fumaça do tabaco); Offering help to quit tobacco use (oferecer ajuda para abandonar o uso do tabaco); Warning about the dangers of tobacco (alertar sobre os perigos do tabaco); Enforcing bans on tobacco advertising (fazer cumprir a proibição da propaganda do tabaco) e Raising taxes on tobacco products (aumentar os impostos dos produtos do tabaco).(6) Apesar dos esforços bem-sucedidos com as políticas antitabaco no Brasil, incluindo a oferta de tratamento no Sistema Único de Saúde,(7,8) há subgrupos de tabagistas com comorbidades relevantes que têm maior dificuldade na cessação tabágica, como os pacientes com DPOC, o que exige esforço adicional na oferta e estratégias dos programas de cessação.(9)
Os tabagistas portadores de doenças crônicas não transmissíveis relacionadas ao uso de tabaco precisam ser tratados com a máxima eficácia, porque, se continuarem fumando, a progressão dessas doenças levará a enormes prejuízos para suas vidas, com incapacidade e mortalidade precoces.(10,11)
A abordagem deve ser direcionada para as mudanças comportamentais, sendo a motivação e o desejo de parar os catalisadores desse processo, apoiada por farmacoterapia eficaz, conforme recomendam as principais diretrizes.(12-14) Os médicos devem estar preparados para tratar esses pacientes, particularmente quando esses já apresentam pneumopatias crônicas.
Os objetivos do presente artigo foram revisar e avaliar as principais evidências do impacto à saúde decorrentes do consumo de tabaco nas doenças respiratórias e alertar o médico, particularmente o pneumologista, de que é preciso priorizar o tratamento do tabagismo na assistência aos pneumopatas.(8,15,16)
METODOLOGIAA estratégia de busca escolhida foi o método denominado revisão integrativa da literatura científica, cujo propósito é o de realizar buscas por palavras-chave, assim como reunir artigos, revisões sistemáticas e relatórios técnicos, de modo a resumir os resultados e evidências acerca de um tema específico.(17-19)
Para a presente revisão foram formuladas as seguintes questões de pesquisa:
- Quais são as evidências do aconselhamento na cessação do tabagismo nos pacientes com doenças respiratórias?
- Quais são as evidências da farmacoterapia na cessação do tabagismo nos pacientes com doenças respiratórias?
- A seleção dos 176 artigos foi efetuada a partir da busca on-line na Biblioteca Virtual em Saúde, SciELO e MEDLINE/PubMed. Foram utilizados os seguintes descritores controlados através de palavras-chave: tabagismo; dependência a nicotina; efeitos à saúde respiratória; farmacoterapia na cessação; aconselhamento na cessação; doença pulmonar obstrutiva crônica; asma; tuberculose; e pneumoconiose.
AVALIAÇÃO CLÍNICA DO TABAGISTA
Os tabagistas com doenças respiratórias apresentam maior necessidade e urgência em parar de fumar; por isso, os médicos precisam assumir um papel proativo no sentido de encorajar e oferecer tratamento para a cessação tabágica. Essa abordagem deve ser realizada em conjunto com o tratamento da doença de base. Para tanto, os médicos necessitam ser capacitados, tanto no manejo da farmacoterapia quanto nas técnicas cognitivo-comportamentais.(13,15)
Desde a primeira visita, o médico deve esclarecer o paciente do fato que parar de fumar será a única medida que resultará na redução do declínio da função pulmonar, melhora da resposta terapêutica e redução da frequência de exacerbações. Essa abordagem deve ser multidisciplinar e alcançar todos os níveis da assistência em saúde, seja ambulatorial, seja hospitalar.(20,21)
A população com doenças respiratórias possui peculiaridades que podem dificultar a cessação tabágica, tais como maior grau de dependência e de sintomas de abstinência; motivação e autoeficácia baixas; excessiva preocupação com ganho ponderal; e elevada prevalência de distúrbio psiquiátrico. Além disso, ela requer tratamento mais intensivo e prolongado.(21,22)
Identificar os fatores preditores e conhecer as técnicas para a cessação tabágica são fundamentais na abordagem do tabagista. A motivação prediz a frequência de tentativas e o grau de dependência prediz o desfecho dessas tentativas. O uso concomitante de álcool e de múltiplas drogas são fatores dificultadores da cessação.(23,24)
O tabagista deve ser submetido à avaliação clínica completa antes de iniciar o tratamento (Quadro 1).(10,13) Os objetivos da anamnese são, dentre outros, analisar o perfil tabágico do paciente; seu grau de motivação, dependência e autoeficácia; sua experiência em tentativas prévias de cessação tabágica; as doenças associadas ao tabagismo; as contraindicações para as medicações específicas; e suas crenças e preferências. (10,25) O médico deve realizar um exame físico completo e solicitar exames de acordo com a demanda e a disponibilidade local.(23) Os resultados da espirometria e de exames de imagem podem ser úteis na motivação para parar de fumar.(24,26,27)

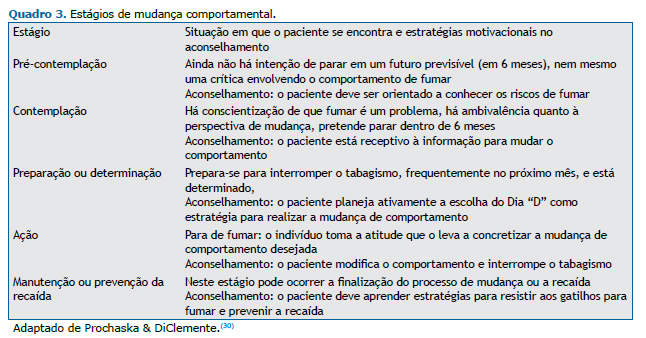
Conhecer o grau de dependência tabágica é importante para guiar o tratamento (Quadro 2). O instrumento mais utilizado é o Teste de Fagerström para Dependência à Nicotina.(28) Em 2012, o teste foi renomeado para Teste de Fagerström para Dependência aos Cigarros. (29) O modelo transteórico de Prochaska e DiClemente é o mais utilizado para avaliar o grau de motivação para a cessação tabágica, sendo útil para programar a tentativa da cessação tabágica (Quadro 3).(30)

EVIDÊNCIAS ATUAIS DA EFETIVIDADE DO ACONSELHAMENTO E DA FARMACOTERAPIA
Aconselhamento cognitivo-comportamental
Após identificar o grau de dependência tabágica de cada paciente, a principal e subsequente ação é o aconselhamento breve para a cessação do tabagismo e a programação de visitas para o acompanhamento, com consultas mais prolongadas.(31)
Sabe-se que a autoeficácia e a autoestima afetam a capacidade de a pessoa parar de fumar; portanto, conselhos construtivos devem ser direcionados para tratar as questões de motivação para deixar de fumar e para prevenir a recaída.(31) Sempre que possível, o médico deve individualizar o tratamento para a cessação do tabagismo, discutindo a relação com o ato de fumar e as razões pelas quais o indivíduo segue fumando, assim como as opções terapêuticas disponíveis (suporte psicológico e farmacológico).(10,13)
No aconselhamento, o médico deve ter empatia, conhecer as estratégias de cessação tabágica e ajudar o tabagista já nessa fase inicial. Deve-se abordar os efeitos negativos do tabagismo e os benefícios de sua cessação.(31) No protocolo de atendimento é fundamental estabelecer a data de cessação; identificar as situações de risco para fumar e treinar habilidades para enfrentá-las; explicar os sintomas de abstinência; e acompanhar o paciente de forma bem próxima por meio de consultas médicas, chamadas telefônicas, e-mails, WhatsApp e SMS.(23,30,31) O médico deve informar sobre possíveis complicações do tratamento e benefícios da cessação. Além disso, reduzir as crenças fatalistas e abordar a depressão melhoram a autoeficácia, a autoestima e o sentimento de controle sobre o tratamento.(31)
Nos pacientes com asma ou DPOC é possível aumentar a motivação usando resultados dos exames espirométricos.(24,26,27) No câncer de pulmão, a postura empática, positiva e direta é fundamental: "Uma das melhores coisas que você pode fazer para combater o câncer de pulmão é parar de fumar. Eu posso ajudar você". Os fumantes com tuberculose melhoram a qualidade de vida quando alocados no protocolo terapêutico Directly Observed Treatment, Short Course (DOTS, tratamento diretamente observado de curta duração) associado ao suporte para a cessação tabágica. Para esses pacientes são indicadas a intervenção breve no momento do diagnóstico e a manutenção do apoio comportamental mensal durante todo o tratamento da tuberculose.(32)
ABORDAGEM FARMACOLÓGICA
Os estudos mostram que, nos pacientes com DPOC, a intervenção farmacológica associada ao aconselhamento comportamental intensivo apresenta efetividade com alta qualidade de evidência através de resultados agrupados em uma meta-análise - risco relativo (RR) = 2,53; IC95%: 1,83-3,50.(33) Em relação à monoterapia, as chances de cessação comparadas ao placebo duplicam com o uso da bupropiona (RR = 2,03; IC95%: 1,26-3,28), mais que duplicam com o uso da terapia de reposição de nicotina (TRN) - RR = 2,60; IC95%: 1,29-5,24 - e triplicam com o uso da vareniclina (RR = 3,34; IC95%: 1,88-5,92).(33)
Em relação ao uso da nortriptilina, fármaco de segunda linha, não há superioridade na cessação em relação ao placebo em pacientes com DPOC.(34) Nos tabagistas com asma, a taxa de cessação é baixa e há ainda poucos estudos. Os possíveis motivos podem incluir a associação ao não desejo de parar de fumar e outros fatores, como depressão, baixo nível socioeconômico e baixa escolaridade.(35) Um ensaio clínico randomizado (ECR) envolvendo pacientes com asma mostrou que não houve diferença na cessação tabágica com o uso de vareniclina em comparação ao de placebo (RR= 1,25; IC95%: 0,38-4,14).(36)
Com o uso de TRN, bupropiona ou vareniclina, como com qualquer outro medicamento, podem ocorrer eventos adversos; portanto, todos os pacientes em uso de fármacos para a cessação tabágica devem ser monitorados. Os Quadros 4 e 5 apresentam os fármacos de primeira linha na cessação do tabagismo e suas principais características.


Tratamento estendido e combinado
Os dados da literatura ainda são escassos para recomendar a utilização de vareniclina de forma estendida. Um estudo observacional aberto, com pacientes com DPOC grave a muito grave e que utilizaram vareniclina por 24 semanas, mostrou que a taxa de abstinência foi de 17,7%, avaliada pela análise de intenção de tratamento.(40) Por outro lado, quando foram avaliados os estudos que incluíram fumantes com características gerais, houve uma demonstração de efetividade de tratamento em relação aos dados agrupados de quatro ECR, envolvendo 2.170 indivíduos (RR = 3,64; IC95%: 2,81-4,72).(32)
Não foram identificados ECR com a utilização de doses reduzidas de vareniclina em pacientes com doenças respiratórias. Existem apenas quatro ECR (total de 1.266 indivíduos) que mostraram, agrupados, que a vareniclina foi efetiva mesmo em doses inferiores àquelas recomendadas para a população de fumantes em geral (RR = 2,08; IC95%: 1,56-2,78).(33) Um estudo retrospectivo envolvendo mais de 14.000 pacientes com diagnóstico de DPOC, com ou sem comorbidades cardiovasculares ou psiquiátricas associadas, mostrou que o uso de bupropiona ou de vareniclina não aumentou o risco de eventos cardiovasculares ou neuropsiquiátricos em seis meses, se comparado aos pacientes sem DPOC que utilizaram TRN.(41)
A combinação de duas formas de TRN apresenta a mesma efetividade quando comparada à vareniclina (OR = 1,06; IC95%: 0,75-1,48).(42) Uma meta-análise com dados agrupados de dois ECR com 787 indivíduos no total mostrou que a combinação de vareniclina com TRN (adesivo) foi mais eficaz quando comparada com o uso de vareniclina isolada (OR = 1,62; IC95%: 1,18-2,23).(43)
TABAGISMO E DOENÇAS RESPIRATÓRIAS
Asma e uso de tabaco
A asma é uma doença fenotipicamente heterogênea, que resulta de interações complexas entre fatores ambientais e genéticos. A exposição à fumaça ambiental de tabaco (FAT), tanto no período pré-natal quanto após o nascimento, está associada a um maior risco de se desenvolver sintomas semelhantes aos da asma na infância.(44,45)
Em uma revisão sistemática com meta-análise,(44) demonstrou-se que a exposição à FAT pré ou pós-natal foi associada a um aumento de 30% a 70% no risco de sibilância incidente, com maior efeito do tabagismo passivo materno pós-natal na sibilância em crianças ≤ 2 anos (OR = 1,70; IC95%: 1,24-2,35) e aumento de 21% a 85% na asma incidente, com efeito mais forte do tabagismo materno pré-natal na asma em crianças com idade ≤ 2 anos (OR = 1,85; IC95%: 1,35-2,53).
Outra revisão sistemática com meta-análise(45) demonstrou que a exposição pré-natal ao tabagismo materno foi associada a um risco aumentado de sibilância em crianças < 6 anos de idade (OR = 1,36; IC95%: 1,19-1,55) e de chiado ou asma em crianças ≥ 6 anos de idade (OR = 1,22; IC95%:1,03-1,44). Um grupo de autores(46) mostrou que as exposições pós-natais ao tabagismo materno ou paterno, respectivamente, foram associadas à sibilância em crianças < 6 anos de idade (OR = 1,21; IC95%: 1,13-1,31; e OR = 1,30; IC95%: 1,13-1,51), embora muitas vezes fosse impossível separar o papel da exposição pós-natal do da exposição pré-natal.
O seguimento de algumas coortes mostrou aumentos nas chances de asma incidente após a cessação do uso de tabaco.(47-49) Em uma dessas coortes o tabagismo continuado ao longo do acompanhamento também aumentou significativamente o risco de asma incidente.(47)
Ainda não há estudos disponíveis que tenham avaliado a mortalidade de asma atribuível ao tabagismo ou a fração de asma atribuível ao tabagismo ativo e/ou passivo no Brasil. Em 2013, 2.047 pessoas morreram por asma no Brasil (5 óbitos/dia), com mais de 120 mil hospitalizações por asma.(50) Nos asmáticos tabagistas, fumar se associa a um acelerado declínio da função pulmonar(51) e a menor resposta à corticoterapia inalatória e sistêmica.(52-55) Além disso, esses pacientes têm menor chance de controlar a doença: asmáticos fumantes apresentam maior frequência de episódios de agudização e maior número de hospitalizações por exacerbações da doença.(56-59)
Desde os anos 1970 já é reconhecida a associação entre o uso de maconha e piora dos sintomas de asma. (60-62) Fumar maconha também causa exacerbações da asma brônquica e aparecimento de sintomas compatíveis com asma.(60-64) A exposição involuntária à fumaça da maconha leva a inalação de substâncias tóxicas, o que piora os sintomas da asma.(65) Assim, os indivíduos com asma ou hiper-reatividade brônquica devem evitar fumar tabaco ou maconha, ou serem expostos passivamente às suas fumaças.
A cessação do tabagismo reduz os sintomas da asma e permite atingir melhor controle da doença.(66,67) Algumas evidências sugerem que os portadores de asma que são fumantes teriam menor probabilidade de parar de fumar do que os fumantes sem asma.(68,69)
Em todo paciente com asma ou hiper-reatividade brônquica, o médico deve indagar o status do tabagismo. No aconselhamento deve enfatizar:
- Asmáticos ou indivíduos com hiper-reatividade brônquica devem evitar fumar ou ficar expostos passiva-mente à fumaça de produtos de tabaco ou maconha
- Os não fumantes devem ser aconselhados a não iniciar o tabagismo
- Fumantes de tabaco ou de maconha devem ser informados a respeito das dificuldades e/ou riscos de manterem o uso desses produtos fumígenos e receber apoio para a cessação do tabagismo e da maconha
- Os principais benefícios da cessação do tabagismo incluem a melhora do controle da asma, a redução das exacerbações e do declínio funcional, além da melhora da resposta terapêutica.
DPOC e uso de tabaco
A DPOC é uma doença inflamatória multissistêmica que resulta da interação entre fatores genéticos e ambientais. Embora a fumaça do cigarro persista como a maior causa da doença, em algumas regiões, a inalação da fumaça da queima de biomassa, as exposições ocupacionais e a poluição atmosférica também têm papel relevante.(70-74)
A carga tabágica tem relação com o desenvolvimento, a progressão e a gravidade da DPOC e usualmente é avaliada pela carga tabágica em anos-maço. Contudo, a duração do tabagismo em anos, além de ser mais fácil para a avaliação, pode ter melhor correlação com o risco de desenvolvimento e progressão da doença.(75)
A prevalência da DPOC varia de acordo com os fatores de riscos e critérios funcionais e analíticos; seu subdiagnóstico ultrapassa a 70%.(76,77) A prevalência da DPOC no mundo e no Brasil é estimada em 12% e 15,8%, respectivamente.(70,78) Como a idade e o tabagismo têm efeito cumulativo, estima-se que 50% dos fumantes desenvolverão a doença ao longo da vida.(79,80)
A DPOC já é a terceira causa de morte no mundo. Um estudo realizado em capitais brasileiras constatou que 65% das mortes atribuíveis ao tabaco são devido a DPOC, doença isquêmica cardíaca, câncer de pulmão e doença cerebrovascular.(81) Em outro estudo brasileiro que comparou as taxas de mortalidade entre 1990 e 2015, constatou-se que houve redução de 31% na taxa de DPOC (de 64,5 para 44,5/100.000 habitantes) e de apenas 2,1% na taxa de câncer de pulmão. Nesse mesmo período, houve redução de 36,1% na taxa de anos de vida perdidos por morte ou incapacidade.(82)
Os pacientes com DPOC costumam omitir de seus médicos que continuam fumando, mesmo quando suas informações sobre o hábito de fumar são confrontadas com medidas de monóxido de carbono ou de cotinina. (83) Os fumantes com DPOC têm maior carga tabágica, maior grau de dependência e recebem mais orientações sobre os riscos e a necessidade de cessar o tabagismo do que os fumantes sem DPOC.(20,84)
A motivação para cessar o tabagismo difere pouco entre os pacientes com e sem DPOC. Contudo, a autoeficácia é menor em fumantes com DPOC, em parte devido à elevada frequência de ansiedade e depressão.(20,70,84) Em uma coorte dinamarquesa de fumantes com DPOC os fatores relacionados com a menor chance de cessação foram idade < 65 anos; obstrução leve ao fluxo aéreo; classificação A da Global Initiative for Chronic Obstructive Lung Disease, pontuação reduzida na escala de Medical Research Council e baixo nível socioeconômico. Naquela coorte, a depressão não piorou a taxa de cessação tabágica, como foi demonstrado em outro estudo.(85)
A cessação do tabagismo é a única intervenção que altera a história natural da DPOC.(20,70,71) Os fumantes com DPOC são mais questionados sobre o tabagismo e recebem mais orientações e tratamento do que os fumantes sem DPOC.(86) Por outro lado, quando eles não são incentivados e encaminhados para programas de cessação, mantêm seus hábitos tabágicos quase inalterados por vários anos.(87) O Quadro 6 sumariza as recomendações terapêuticas e os benefícios na cessação do tabagismo nos pacientes com DPOC.

Câncer de pulmão e uso de tabaco
A fumaça do cigarro contém mais de 7.000 compostos. (93) Segundo avaliação da Agência Internacional de Pesquisa em Câncer, mais de 60 agentes são considerados carcinogênicos em animais de laboratórios, dos quais, em 12 deles, há evidências suficientes de carcinogenicidade para humanos.(94,95) Há uma forte correlação entre o consumo de cigarros ao longo da vida e as alterações genéticas que levam à perda do mecanismo de supressão tumoral (metilação do DNA e as alterações de microRNA).(71,96-98) O tabagismo ativo e o fumo passivo são responsáveis por mais de 90% dos casos de câncer de pulmão, com relação direta entre o aumento do risco de câncer e o consumo de tabaco calculado em anos-maço.(71,97)
Estudos brasileiros revelaram elevadas incidência e mortalidade de câncer atribuíveis ao tabagismo, particularmente os de pulmão, cavidade oral e laringe. (99,100) Um estudo que avaliou a fração de câncer atribuída a fatores de risco modificáveis no Brasil estimou que, até 2020, a fração atribuível de carga de câncer de pulmão relacionada ao tabagismo na população será de 83,28% em homens e de 64,80% em mulheres.(100,101)
Uma revisão sistemática(102) de estudos com portadores de câncer de pulmão com tumores não pequenas células, em estágio inicial, e que seguiram fumando mostrou RR = 2,94 e IC95%: 1,15-7,54 para mortalidade por todas as causas e RR = 1,86 e IC95%: 1,01-3,41 para recidiva. Nos portadores de o tumores de pequenas células, com doença limitada e que persistiram fumando, o risco relativo de mortalidade por todas as causas (RR = 1,86; IC95%:1,33-2,59); para um segundo tumor primário (RR = 4,31; IC95%: 1,09-16,98); e para recidiva (RR = 1,26; IC95%: 1,06-1,50). A sobrevida dos pacientes com tumores não pequenas células com idade ≥ 65 anos foi de 33% para aqueles que continuaram fumando e de 70% para aqueles que pararam de fumar. A sobrevida em 5 anos no grupo com tumores pequenas células foi de 29% entre fumantes e de 63% nos que pararam de fumar.(102)
O tabagista com câncer convive com pressões médicas, familiares e pessoais para a cessação tabágica e sente culpa pelo surgimento da doença, embora deseje parar na maioria dos casos. A ameaça de morte e de sofrimentos físicos e psíquicos, assim como os desafios futuros, dificulta a tomada de decisão de alguns pacientes e impulsionam outros para a cessação. O pensamento distorcido de ser tarde para abandonar o cigarro atrapalha o processo.(103)
Um mesmo paciente oscila entre momentos de alta ou baixa autoeficácia para deixar de fumar. É preciso sensibilidade do médico para observar a diferença e promover uma abordagem individualizada com foco nos benefícios da cessação tabágica, o que possibilitará melhores resultados no desfecho do tratamento.(103-105) Cerca de 50% dos fumantes diagnosticados com câncer permanecem fumando.(106) Os fumantes com câncer de pulmão apresentam maior motivação para deixar de fumar do que a população geral; contudo, podem exigir cuidados mais intensivos e abrangentes.(103)
O tabagismo é um fator prognóstico independente, o único sob controle direto do paciente. As taxas de abstinência são elevadas logo após conhecer o diagnóstico, mas as de recaída também. O tratamento e a prevenção da recaída são imperativos desde a primeira consulta.(103) O Quadro 7 sumariza as principais recomendações na abordagem do tratamento do tabagismo, assim como enfatiza os benefícios da cessação durante a terapêutica oncológica.

Tuberculose e uso de tabaco
Em 2016, 10,4 milhões de pessoas adoeceram e 1,7 milhões morreram devido à tuberculose; mais de 95% dos óbitos por tuberculose ocorreram em países de baixa e média renda.(110) O Brasil encontra-se entre os 22 países que concentram 80% dos casos de tuberculose no mundo. Segundo o Ministério da Saúde, houve 4.374 mortes por tuberculose no Brasil em 2014.(111) Tanto a tuberculose quanto o tabagismo são mais comuns nas populações de países de baixa a média renda. Segundo a Organização Mundial da Saúde, mais de 20% da incidência global de tuberculose pode ser atribuída ao tabagismo.(112)
Há um século, o tabagismo já era identificado como um fator de risco para a tuberculose.(113) Na última década, vários estudos vêm demonstrando uma significativa associação entre exposição à fumaça do tabaco e tuberculose, após ajuste para outros fatores de risco.(114) Há evidências da associação de tabagismo (ativo e passivo) com tuberculose ativa, assim como com a resposta terapêutica, recaídas e mortalidade por tuberculose.(71,112,114-116) Esses efeitos parecem ser independentes de outros fatores de risco de tuberculose, como o alcoolismo e condições socioeconômicas.(71,112,114)
A fumaça do tabaco prejudica a defesa pulmonar através de mudanças estruturais, e alterações celulares e da resposta imune. Fumar compromete a integridade do epitélio das vias respiratórias, altera o clearance mucociliar e reduz a capacidade fagocitária dos macrófagos alveolares, o que aumenta a probabilidade de que o Mycobacterium tuberculosis atinja os alvéolos, onde se inicia a infecção por tuberculose.(71,117-121) Alguns estudos sugerem que o aumento da suscetibilidade à tuberculose pulmonar se deva à redução de imunoglobulinas circulantes e da relação CD4/CD8, ambas causadas pela fumaça do tabaco.(71,122-126)
O tabagismo passivo aumenta tanto o risco de infecção por tuberculose quanto à ocorrência da tuberculose ativa, especialmente em crianças. Esse risco pode estar aumentado em nove vezes em crianças e jovens menores de 15 anos, mesmo sem contato com tuberculose pulmonar no domicilio. Existe uma forte relação dose-resposta entre o risco de tuberculose e o número de cigarros aos quais as crianças são expostas por dia.(127,128) Adultos não tabagistas expostos à fumaça de tabaco em ambientes fechados também apresentam um risco aumentado de desenvolver tuberculose pulmonar.(129) Comparados aos não fumantes, os tabagistas com tuberculose apresentam risco aumentado de manifestações clínicas mais severas; mortalidade; retardo na negativação do escarro; falência no tratamento; recaída da tuberculose; resistência a medicamentos tuberculostáticos; lesões cavitárias; maior positividade no escarro; e sequelas mais extensas.(71,114,115,124,130-133)
Os tabagistas portadores de tuberculose ativa mas sem história anterior de tuberculose apresentam um risco de morte nove vezes maior por tuberculose quando comparados a portadores de tuberculose que nunca fumaram.(134)
O controle do tabagismo é uma importante estratégia para reduzir o número de pacientes infectados com o bacilo da tuberculose e também de pessoas que irão desenvolver a doença. Para tanto, torna-se fundamental aconselhar e apoiar os fumantes com tuberculose a cessar o tabagismo. Os tabagistas com tuberculose, quando param de fumar, reduzem o risco de morte por tuberculose em cerca de 65% em comparação com os que continuam a fumar.(134) A Organização Mundial da Saúde recomenda que os programas de controle da tuberculose e do tabagismo trabalhem de forma integrada para que o tratamento do tabagismo seja oferecido a todo paciente com tuberculose.(112,114,115)
Doenças respiratórias ambientais e uso de tabaco
O tabagismo, a poluição do ar ambiental e a poluição intradomiciliar são fatores de risco que ocupam, respectivamente, o segundo (7,13 milhões de mortes/ano), o sexto (4,3 milhões de mortes/ano) e o oitavo (2,6 milhões de mortes/ano) lugares no ranking para a mortalidade global.(135) No Brasil, a poluição do ar ambiental ocupa o 11º lugar no ranking.(136)
As doenças relacionadas a material particulado, gases e agentes cancerígenos ocorrem em virtude do estresse oxidativo, inflamação pulmonar e sistêmica e lesão no DNA. As principais doenças relacionadas com a exposição a poluentes ambientais são as doenças cardiovasculares isquêmicas, neoplasias, DPOC e infecções respiratórias.(137)
Segundo estimativas da Organização Mundial da Saúde para 2016, a poluição do ar ambiental e a poluição intradomiciliar, no Brasil, foram responsáveis, respectivamente, por mais de 51,8 mil e 14,1 mil mortes, com taxa de mortalidade padronizada de 24 e de 7 óbitos/100 mil habitantes.(138) Um grupo de autores, estimando o material particulado inalado em 12 mg/cigarro e a exposição à poluição do ar entre 13-30 µm³ de ar/dia, avaliaram que há riscos para câncer de pulmão, doenças cardiovasculares e doenças pulmonares.(139)
Outro grupo de autores encontrou menores valores da função pulmonar em mulheres fumantes e não fumantes que moravam em ambientes com maiores níveis de poluição em relação aos controles. A exposição de fumantes à FAT aumenta o risco de câncer de pulmão, evidenciando um efeito aditivo entre os riscos.(140)
Não foram identificadas diferenças entre o perfil de fumantes e as doenças relacionadas à poluição do ar. Embora ainda não seja conhecido o impacto isolado da cessação de tabagismo em indivíduos expostos à poluição, a proibição de fumar em ambientes fechados teve um relevante impacto na redução da morbidade e mortalidade. Uma meta-análise com 44 estudos revelou importantes reduções na hospitalização e em óbitos por doenças respiratórias.(141) Esse fato permite inferir que as pessoas vivendo numa mesma cidade, sem mudanças dos níveis de poluição, poderiam se beneficiar da redução da exposição à FAT. O mesmo vale para o impacto da cessação do tabagismo na redução das doenças respiratórias observada em estudos de coorte.(142)
Doenças respiratórias ocupacionais e uso de tabaco
A dupla exposição, ao tabaco e ocupacional, tem relação somativa de efeitos deletérios e, algumas vezes, sinérgicas, potencializando as agressões às vias aéreas e ao interstício pulmonar. A inibição do clearance mucociliar e as demais alterações nas vias aéreas resultam em maior retenção de partículas inaladas, bem como facilita a agressão por gases, névoas ou vapores químicos inalados. A inflamação e a toxicidade no DNA de ambas as exposições podem aumentar o risco de adoecimento.(97,143,144)
Os ambientes de trabalho são importantes fatores de risco para morbidade e mortalidade globais, sendo estimados em 1,53 milhões o número de óbitos/ano e em 75,93 milhões o número de anos de vida perdidos por morte ou incapacidade provocados pelos diversos riscos ocupacionais.(145) Segundo dados da carga global de doenças em 2016, a exposição à fumaça ambiental do tabaco nos ambientes de trabalho, isoladamente, esteve associada a 433,2 mil óbitos, com maior impacto na mortalidade por doenças isquêmicas cardiovasculares (252 mil), seguido por DPOC (52 mil) e câncer de pulmão (44,4 mil).(146)
A prevalência de fumantes entre os trabalhadores varia com o tipo de empresa e de atividade desempenhada pelos mesmos, sendo menor em trabalhadores da saúde e educação e mais elevada em trabalhadores da indústria, serviços de limpeza, mineração e construção.(147) Nesses últimos grupos de trabalhadores, a prevalência é mais alta do que na população geral, com taxas encontradas, comparando a prevalência populacional com a dos trabalhadores, de 40,2% vs. 53,2% na China,(148) 43,0% vs. 66,3% na Turquia(149) e 15,1% vs. 49,8% no Brasil.(150) Essas altas taxas revelam o impacto do tabagismo entre os menos escolarizados e com menor renda, que integram a força de trabalho em atividades mais insalubres ou exposta a maiores riscos nos ambientes de trabalho.
A cessação de tabagismo reduz o risco de morbidade e mortalidade, sendo maior o benefício quanto mais precoce for a idade da cessação.(151) É recomendável que os serviços de saúde ocupacional das empresas, desde o ingresso do trabalhador, desenvolvam políticas para estimular e apoiar o trabalhador fumante e sua família a parar de fumar. Oferecer tratamento aos pacientes tabagistas deve ser um procedimento adotado nos serviços de atenção primária à população e nas empresas.(152)
A realização de pesquisas com questionários breves para monitorar a relação saúde/doença, além de ajudar a detectar a necessidade de intervenções nos ambientes de trabalho, pode criar importantes momentos motivacionais, aumentando assim a chance de sucesso na cessação tabágica. Entre os diversos fatores motivadores da cessação apresentados por esses grupos de trabalhadores mais expostos e mais vulneráveis socialmente, destacam-se a presença de sintomas respiratórios ou de doença respiratória já estabelecida.(149)
Doenças respiratórias intersticiais e uso de tabaco
Nos últimos anos, a preocupação com os malefícios do tabagismo começou a se concentrar no desenvolvimento das doenças pulmonares intersticiais (DPI), sendo três patologias consideradas etiologicamente ligadas ao tabagismo(153): DPI associada à bronquiolite respiratória; pneumonia intersticial descamativa; e histiocitose pulmonar de células de Langerhans.
Algumas doenças intersticiais são mais propensas a se desenvolver em fumantes, como a fibrose pulmonar idiopática e a DPI associada à artrite reumatoide.(153) Alguns indivíduos também podem desenvolver uma combinação de fibrose pulmonar e enfisema. Essa associação é considerada um fenótipo distinto da fibrose pulmonar idiopática.(154)
A identificação do papel do tabagismo nas DPI é importante porque a compreensão das vias patogênicas poderia permitir o desenvolvimento de novos medicamentos. Do ponto de vista clínico, o reconhecimento de um fenótipo relacionado ao tabagismo facilitaria o diagnóstico e o tratamento precoces.(155)
Um grupo de autores(156) analisou quatro estudos de coorte prospectivos, com 11.691 participantes no total, e avaliou a mortalidade em indivíduos com anormalidades pulmonares intersticiais. As lesões foram associadas a maior carga tabágica em dois desses estudos e a maior taxa de mortalidade em todas as coortes.
As DPI relacionadas ao tabaco são menos reconhecidas, mas existe uma correlação causal bem definida, baseada em dados epidemiológicos. A cessação do tabagismo é a terapia fundamental para o controle desses pacientes, e sua abordagem requer a perfeita integração dos dados clínicos, funcionais, radiológicos e histopatológicos.
Doenças respiratórias infecciosas e uso de tabaco
A deposição dos agentes tóxicos da fumaça do tabaco nas vias aéreas afeta os mecanismos de defesa em múltiplos níveis: redução do transporte mucociliar, maior aderência bacteriana no epitélio respiratório; e aumento da permeabilidade vascular alveolar e epitelial.(157) Além disso, a contínua exposição ao tabaco associa-se a importantes modificações na microflora nasofaríngea, o que favorece a colonização por patógenos oportunistas.(158)
Um estudo experimental demonstrou que a exposição crônica à FAT aumentou os níveis de citocinas inflamatórias e TNF-α nos pulmões, e prejudicou a imunidade adaptativa após infecção crônica ou imunização intranasal com a proteína recombinante P6 para Haemophilus influenzae em camundongos. Os autores concluíram que há evidências inequívocas de que a exposição à FAT possui efeitos em longo prazo que são prejudiciais sobre o microambiente inflamatório pulmonar, a imunidade à infecção e a resposta à vacinação.(159)
Uma revisão sistemática mostrou que tabagistas tinham maior risco de contrair pneumonia bacteriana do que ex-fumantes - hazard ratio (HR, razão de risco) = 1,37; IC95%: 1,06-1,78 - e do que os não-fumantes - HR = 1,73; IC95%: 1,44-2,06. (160) A pneumonia e a influenza aumentam o risco de morbidade e mortalidade e, quando o indivíduo é fumante, elevam ainda mais os custos médico-sociais e previdenciários. Um estudo de 2017 demonstrou que a pneumonia é a terceira causa de adoecimento relacionado ao tabagismo no Brasil.(2) Em síntese, de acordo com as evidências científicas, o Quadro 8 demonstra a exposição e riscos dos tabagistas.

Hospitalizados com doenças respiratórias e uso de tabaco
Estudos sobre a prevalência de tabagismo em pacientes hospitalizados no Brasil variaram entre 15% e 22% (167,168) Em um estudo,(169) os autores encontraram uma prevalência de tabagismo de 25% entre pacientes internados em um hospital livre de tabaco, e 55% apresentavam sintomas de abstinência. Em uma revisão sistemática, encontrou-se de 15% a 27% de tabagistas entre pacientes hospitalizados.(170)
A internação é uma janela de oportunidade para iniciar a abordagem antitabágica com grande chance de sucesso, principalmente se houver acompanhamento após a alta hospitalar.(12,169) A abordagem do tabagista internado deve estar inserida na rotina hospitalar. Apesar de esse paciente apresentar muitas vezes uma motivação elevada e estar disponível, apenas uma minoria recebe tratamento para a cessação tabágica e a maior parte recai logo após a alta hospitalar.(12,169)
A conduta recomendada é que seja oferecido aconselhamento durante a internação e seguimento por, pelo menos, quatro semanas, seja presencial, seja por contato telefônico. Em uma meta-análise(171) com 50 estudos, concluiu-se que as abordagens intensivas seguidas por acompanhamento após a alta tiveram maior efetividade, pois as recaídas ocorrem principalmente durante o primeiro mês após a alta. Identificar a fissura e outros fatores que indiquem maior chance de fracasso, como a dependência ao álcool ou a outras drogas, permite que se possa individualizar o tratamento daqueles com maior risco de recaídas.
Foi avaliada a eficácia de um programa de cessação para hospitalizados por doença respiratória (doenças respiratórias) ou doença cardíaca e registrou-se que 31% dos pacientes com doenças respiratórias estavam abstinentes seis meses após alta hospitalar.(172) Os pacientes que receberam aconselhamento individual e medicação durante a internação e após a alta apresentaram maior adesão ao tratamento, inclusive após a alta hospitalar.(173)
O momento da internação deve ser transformado em oportunidade de cessação do tabagismo. Os tabagistas hospitalizados com doenças respiratórias devem ser orientados sobre os benefícios dessa cessação e avaliados quanto a seu grau de motivação e dependência para receber tratamento específico, o que é similar ao recomendado para pacientes com outras patologias. Programas com equipes treinadas em tabagismo apresentam boa relação custo-efetividade na abordagem dos tabagistas.(174) O acompanhamento após a alta, por pelo menos seis meses, melhora os desfechos e o sucesso da abstinência.(170,175,176) A intervenção intensiva associada ao tratamento farmacológico para a cessação tabágica nos pacientes com doença respiratória, iniciado ainda durante a hospitalização, é eficaz, com grau de evidência de alta qualidade.(22)
CONSIDERAÇÕES FINAIS
Todos os pacientes com doenças respiratórias devem ser questionados se fumam, incentivados a parar de fumar e encaminhados para a cessação tabágica, independentemente de sua idade e estágio da doença. A cessação do tabagismo, com base na terapia cognitivo-comportamental e farmacoterapia, é a primeira medida a ser tomada no tratamento das pneumopatias e resulta em importantes benefícios, tais como redução das exacerbações e hospitalizações; redução dos sintomas respiratórios; melhora da qualidade de vida; redução das limitações para as atividades diárias; melhora do controle das comorbidades; melhora da resposta aos broncodilatadores e corticoides inalatórios; maiores chances de sobrevida; menor risco de recidiva e de incidência de segundo tumor primário relacionado ao tabaco; maior controle da dor; elevação da autoestima; e menores riscos de complicações da cirurgia, da radioterapia e da quimioterapia.
REFERÊNCIAS
1. World Health Organization [homepage on the Internet]. WHO, Geneva; Fact Sheet [updated 2018 Mar 9, cited 2018 Aug 26]. Tobacco [about 8 screens]. Available from: http://www.who.int/en/news-room/fact-sheets/detail/tobacco
2. Instituto de Efectividad Clínica y Sanitaria; Instituto Nacional do Câncer; Fundação Oswaldo Cruz [homepage on the Internet], ACT Promoção da Saúde [updated 2017 May 31, cited 2018 Aug 26]. Carga de doença atribuível ao uso do tabaco no Brasil e potencial impacto do aumento de preços por meio de impostos [about 2 screens]. Available from http://actbr.org.br/post/carga-de-doenca-atribuivel-ao-uso-do-tabaco-no-brasil-e-potencial-impacto-do-aumento-de-precos-por-meio-de-impostos/16952/
3. Brasil. Ministério da Saúde [homepage on the Internet]. Brasília: o Ministério; c2018 [cited 2018 Aug 26]. Vigitel Brasil 2017--Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito. [Adobe Acrobat document, 132 p.]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/vigitel_brasil_2017_vigilancia_fatores_riscos.pdf
4. Brasil. Instituto Brasileiro de Geografia e Estatística [homepage on the Internet]. São Paulo: IBGE; c2018 [cited 2018 Aug 26]. Projeção da População do Brasil e das Unidades de Federação. Available from: https://www.ibge.gov.br/apps/populacao/projecao/
5. Instituto Nacional do Câncer José Alencar Gomes da Silva (INCA) [homepage on the Internet]. Rio de Janeiro: INCA; c2012 [cited 2018 Aug 26]. Convenção-quadro para o controle do tabaco: texto oficial, 2011. [Adobe Acrobat document, 58p]. Available from http://www.saude.pr.gov.br/arquivos/File/convencao_quadro_texto_oficial.pdf
6. World Health Organization. WHO Report on the Global Tobacco Epidemic, 2008: The MPOWER. Geneva: World Health Organization; 2008.
7. Levy D, de Almeida LM, Szklo A. The Brazil SimSmoke policy simulation model: the effect of strong tobacco control policies on smoking prevalence and smoking-attributable deaths in a middle income nation. PLoS Med. 2012;9(11):e1001336. https://doi.org/10.1371/journal.pmed.1001336
8. Instituto Nacional do Câncer José Alencar Gomes da Silva (INCA) [homepage on the Internet]. Rio de Janeiro: INCA; c2018 [cited 2018 Aug 26]. Programa Nacional de Controle do Tabagismo [about 5 screens]. Available from: http://www2.inca.gov.br/wps/wcm/connect/acoes_programas/site/home/nobrasil/programa-nacional-controle-tabagismo
9. Araujo AJ. Tratamento do tabagismo pode impactar a DPOC. Pulmao RJ - Atualizações Temáticas. 2009;1(1):20-33. http://www.sopterj.com.br/wp-content/themes/_sopterj_redesign_2017/_revista/atualizacao_tematica/03.pdf
10. Corrêa da Silva LC, Araújo AJ, Queiroz ÂM, Sales MD, Castellano MV; Comissão de Tabagismo da SBPT. Smoking control: challenges and achievements. J Bras Pneumol. 2016;42(4):290-298. http://www.jornaldepneumologia.com.br/detalhe_artigo.asp?id=2566
11. Schmidt MI, Duncan BB, Azevedo e Silva G, Menezes AM, Monteiro CA, Barreto SM, et al. Chronic non-communicable diseases in Brazil: burden and current challenges. Lancet. 2011;377(9781):1949-61. [cited 2018 Aug 26]. Available from: https://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736(11)60135-9.pdf
12. Reichert J, Araujo AJ, Gonçalves CM, Godoy I, Chatkin JM, Sales MP, et al. Smoking cessation guidelines--2008. J Bras Pneumol. 2008;34(10):845-80. http://jornaldepneumologia.com.br/detalhe_artigo.asp?id=817
13. Fiore MC, Jaén CR, Baker TB, Bailey WC, Benowitz NL, Curry SJ, et al. Treating Tobacco Use and Dependence: 2008 Update--Clinical practice guideline. Rockville: US Department of Health and Human Services; 2008. https://www.ncbi.nlm.nih.gov/books/NBK63952/
14. Tønnesen P. Smoking cessation and COPD. Eur Respir Rev. 2013;22(127):37-43. http://err.ersjournals.com/content/errev/22/127/37.full.pdf
15. Sociedade Brasileira de Pneumologia e Tisiologia. Manual de Condutas e Práticas em Tabagismo. São Paulo: AC Farmacêutica; 2012.
16. Hoogendoorn M, Feenstra TL, Hoogenveen RT, Rutten-van Mölken MP. Long-term effectiveness and cost-effectiveness of smoking cessation interventions in patients with COPD. Thorax. 2010 Aug;65(8):711-8. https://thorax.bmj.com/content/thoraxjnl/65/8/711.full.pdf
17. Mendes KDS, Silveira RCCP, Galvão CM. Revisão integrativa: método de pesquisa para a incorporação de evidências na saúde e na enfermagem. Texto & Contexto Enfermagem. 2008;17(4):758-64.
18. Grant MJ, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies Health Info Libr J. 2009 Jun;26(2):91-108. http://dx.doi.org/10.1111/j.1471-1842.2009.00848.x
19. Broome ME. Integrative literature reviews for the development of concepts. In: Rodgers BL, Knafl KA, editors. 2nd ed. Concept Development in Nursing. Philadelphia, PA: W. B. Saunders Co., 1993. p. 231-250.
20. Jiménez-Ruiz CA, Andreas S, Lewis KE, Tonnesen P, van Schayck, Hajek P, Tonstad S., et al. Statement on smoking cessation in COPD and other pulmonary diseases and in smokers with comorbidities who find it difficult to quit. Eur Respir J. 2015;46(1):61-79. http://erj.ersjournals.com/content/46/1/61
21. Arancibia F. Enfermedad Pulmonar Obstructiva Crónica y Tabaquismo. Rev Chil Enferm Respir. 2017;33(3):225-229. https://scielo.conicyt.cl/scielo.php?script=sci_arttext&pid=S0717-73482017000300225
22. Jiménez Ruiz CA, Buljubasich D, Riesco Miranda JA, Acuña Iscaray A, da Granda Orive JI, Chatkin JM, et al. Using PICO Methodology to Answer Questions About Smoking in COPD Patients. Arch Bronconeumol. 2017;53(11):622-628. Available from: http://dx.doi.org/10.1016/j.arbres.2017.04.012
23. Ussher M, Kakar G, Hajek P, West R. Dependence and motivation to stop smoking as predictors of success of a quit attempt among smokers seeking help to quit. Addict Behav. 2016;53:175-80. https://core.ac.uk/download/pdf/82759925.pdf
24. Martin-Lujan F, Piñol-Moreso JLI, Martin-Vergara NM, Basora-Gallisa J, Pascual-Palacios I, et al. Effectiveness of a structured motivational intervention including smoking cessation advice and spirometry information in the primary care setting: the ESPITAP study. BMC Public Health. 2011;11:859. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3236011/pdf/1471-2458-11-859.pdf
25. Hughes JR, Naudb S. Perceived role of motivation and self-efficacy in smoking cessation: A secondary data analysis. Addict Behav. 2016;61:58-61. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4943656/pdf/nihms791085.pdf
26. Irizar-Aramburu MI, Martínez-Eizaguirre JM, Pacheco-Bravo, Diaz-Atienza M, Aguirre-Arratibel I, et al. Effectiveness of spirometry as a motivational tool for smoking cessation: a clinical trial, the ESPIMOAT study. BMC Fam Pract. 2013,14:185. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4028857/pdf/1471-2296-14-185.pdf
27. Parker DR, Eltinge S, Rafferty C, Eaton CB, Clarke J, Goldman RE. Primary care providers' views on using lung age as an aid to smoking cessation counseling for patients with chronic obstructive pulmonary disease. Lung. 2015;193(3):321-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4433592/pdf/nihms673990.pdf
28. Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström Test for Nicotine Dependence: a revision of the Fagerström Tolerance Questionnaire. Br J Addict. 1991;86(9):1119-27. https://pdfs.semanticscholar.org/74c8/dd44c488807e054a5ed8711f6bc7b2fbeaea.pdf
29. Fagerström K. Determinants of tobacco use and renaming the FTND to the Fagerström Test for Cigarette Dependence. Nicotine Tob Res. 2012;14(1):75-8. https://nicotinepolicy.info/documents/research/Fager%20Determin%20Renaming%20FTND.pdf
30. Prochaska JO, DiClemente CC. Transtheoretical therapy: Toward a more integrative model of change. Psych Theory Res Pract. 1982;19(3):276-88. http://dx.doi.org/10.1037/h0088437
31. Masefield S, Powell P, Jiménez-Ruiz C, Hajek P, Lewis K, Andreas S, et al. Recommendations to improve smoking cessation outcomes from people with lung conditions who smoke. ERJ Open Res. 2016;2(2). pii: 00009-2016. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5005168/
32. Awaisu A, Nik Mohamed MH, Mohamad Noordin N, Abd Aziz N, Syed Sulaiman SA, Muttalif AR, et al. The SCIDOTS Project: evidence of benefits of an integrated tobacco cessation intervention in tuberculosis care on treatment outcomes. Subst Abuse Treat Prev Policy. 2011;6:26. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3196696/pdf/1747-597X-6-26.pdf
33. van Eerd EAM, van der Meer RM, van Schayck OC, Kotz D. Smoking cessation for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;(8):CD010744. https://www.ncbi.nlm.nih.gov/pubmed/27545342
34. Wagena EJ, Knipschild PG, Huibers MJ, Wouters EF, van Schayck CP. Efficacy of bupropion and nortriptyline for smoking cessation among people at risk for or with chronic obstructive pulmonary disease. Arch Intern Med. 2005;165(19):2286-92. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/486760
35. Chatkin JM, Dullius CR. The management of asthmatic smokers. Asthma Res Pract. 2016;2:10. https://asthmarp.biomedcentral.com/track/pdf/10.1186/s40733-016-0025-7
36. Cahill K, Lindson-Hawley N, Thomas KH, Fanshawe TR, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2016;(5):CD006103. https://www.ncbi.nlm.nih.gov/pubmed/27158893
37. European Network for Smoking and Tobacco Prevention (ENSP) [homepage on the Internet]. Brussels: ENSP; c2016 [cited 2018 Sep 2]. ENSP Guidelines for treating tobacco dependence. [Adobe Acrobat document, 156 p.]. Available from: http://elearning-ensp.eu/assets/English%20version.pdf
38. Brasil. Ministério da Saúde [homepage on the Internet]. Brasília: Ministério da Saúde; c2015 [cited 2018 Sept 2]. Estratégias para cuidado da pessoa com doença crônica: o cuidado da pessoa tabagista. Cad Atenção Básica. 2015;40. [Adobe Acrobat document, 156 p.]. Available from: http://189.28.128.100/dab/docs/portaldab/publicacoes/caderno_40.pdf
39. National Comprehensive Cancer Network (NCCN) [homepage on the Internet]. Brussels: NCCN; c2017 [updated 2017 Aug 21; cited 2018 Sept 2]. Clinical Practice Guidelines in Oncology (NCCN Guidelines). Smoking Cessation. [Adobe Acrobat document, 66 p.]. Available from: http://oncolife.com.ua/doc/nccn/Smoking_Cessation.pdf
40. Jiménez-Ruiz CA, Garcia Rueda M, Martinez Muñiz MA, Sellarés J, Jiménez-Fuentes MA, Lázaro Asegurado L, et al. Varenicline in smokers with severe or very severe COPD after 24 weeks of treatment. A descriptive analysis: VALUE study. Monaldi Arch Chest Dis. 2017;87(3):874. Available from: https://www.monaldi-archives.org/index.php/macd/article/view/874/801
41. Kotz D, Viechtbauer W, Simpson CR, van Schayck OCP, West R, Sheikh A. Cardiovascular and neuropsychiatric risks of varenicline and bupropion in smokers with chronic obstructive pulmonary disease. Thorax. 2017;72(10):905-911. Available from: https://thorax.bmj.com/content/72/10/905
42. Cahill K, Stevens S, Perera R, Lancaster T. Pharmacological interventions for smoking cessation: an overview and network meta-analysis. Cochrane Database Syst Rev. 2013(5):CD009329. Available from: http://tobacco.cochrane.org/sites/tobacco.cochrane.org/files/public/uploads/UKNSCC%202015%20summaries-%20pharmacological.pdf
43. Chang PH, Chiang CH, Ho WC, Wu PZ, Tsai JS, Guo FR. Combination therapy of varenicline with nicotine replacement therapy is better than varenicline alone: a systematic review and meta-analysis of randomized controlled trials. BMC Public Health. 2015;15:689. Available from: https://bmcpublichealth.biomedcentral.com/track/pdf/10.1186/s12889-015-2055-0
44. Burke H, Leonardi-Bee J, Hashim A, Pine-Abata H, Chen Y, Cook DG, et al. Prenatal and passive smoke exposure and incidence of asthma and wheeze: systematic review and meta-analysis. Pediatrics. 2012;129(4):735-44. https://doi.org/10.1542/peds.2011-2196
45. Gilliland FD, Berhane K, Li YF, Rappaport EB, Peters JM. Effects of early onset asthma and in utero exposure to maternal smoking on childhood lung function. Am J Respir Crit Care Med. 2003;167(6):917-24. https://doi.org/10.1164/rccm.200206-616OC
46. Silvestri M, Franchi S, Pistorio A, Petecchia L, Rusconi F. Smoke exposure, wheezing, and asthma development: a systematic review and meta-analysis in unselected birth cohorts. Pediatr Pulmonol. 2015;50(4):353-62. https://doi.org/10.1002/ppul.23037
47. Godtfredsen NS, Lange P, Prescott E, Osler M, Vestbo J. Changes in smoking habits and risk of asthma: a longitudinal population based study. Eur Respir J. 2001;18(3):549-54. https://doi.org/10.1183/09031936.01.00100801
48. Polosa R, Knoke JD, Russo C, Piccillo G, Caponnetto P, Sarvà M, et al. Cigarette smoking is associated with a greater risk of incident asthma in allergic rhinitis. J Allergy Clin Immunol. 2008;121(6):1428-34. https://doi.org/10.1016/j.jaci.2008.02.041
49. Nakamura K, Nagata C, Fujii K, Kawachi T, Takatsuka N, Oba S, et al. Cigarette smoking and the adult onset of bronchial asthma in Japanese men and women. Ann Allergy Asthma Immunol. 2009;102(4):288-93. https://doi.org/10.1016/S1081-1206(10)60333-X
50. Cardoso TA, Roncada C, Silva ERD, Pinto LA, Jones MH, Stein RT, et al. The impact of asthma in Brazil: a longitudinal analysis of data from a Brazilian national database system. J Bras Pneumol. 2017;43(3):163-168. https://doi.org/10.1590/s1806-37562016000000352
51. Lange P, Parner J, Vestbo J, Schnohr P, Jensen G. A 15-year follow-up study of ventilatory function in adults with asthma. N Engl J Med. 1998;339(17):1194-200. https://doi.org/10.1056/NEJM199810223391703
52. Zheng X, Guan W, Zheng J, Ye P, Liu S, Zhou J, et al. Smoking influences response to inhaled corticosteroids in patients with asthma: a meta-analysis. Curr Med Res Opin. 2012;28(11):1791-8. https://doi.org/10.1185/03007995.2012.722991
53. Chalmers GW, Macleod KJ, Little SA, Thomson LJ, McSharry CP, Thomson NC. Influence of cigarette smoking on inhaled corticosteroid treatment in mild asthma. Thorax. 2002;57(3):226-30. https://doi.org/10.1136/thorax.57.3.226
54. Lazarus SC, Chinchilli VM, Rollings NJ, Boushey HA, Cherniack R, Craig TJ, et al. Smoking affects response to inhaled corticosteroids or leukotriene receptor antagonists in asthma. Am J Respir Crit Care Med. 2007;175(8):783-90. https://doi.org/10.1164/rccm.200511-1746OC
55. Chaudhuri R, Livingston E, McMahon AD, Thomson L, Borland W, Thomson NC. Cigarette smoking impairs the therapeutic response to oral corticosteroids in chronic asthma. Am J Respir Crit Care Med. 2003;168(11):1308-11. https://doi.org/10.1164/rccm.200304-503OC
56. Boulet LP, FitzGerald JM, McIvor RA, Zimmerman S, Chapman KR. Influence of current or former smoking on asthma management and control. Can Respir J. 2008;15(5):275-9. https://doi.org/10.1155/2008/725074
57. Thomson NC, Chaudhuri R. Asthma in smokers: challenges and opportunities. Curr Opin Pulm Med. 2009;15(1):39-45. https://doi.org/10.1097/MCP.0b013e32831da894
58. Chaudhuri R, McSharry C, McCoard A, Livingston E, Hothersall E, Spears M, et al. Role of symptoms and lung function in determining asthma control in smokers with asthma. Allergy. 2008;63(1):132-5. https://doi.org/10.1111/j.1398-9995.2007.01538.x
59. U.S. Department of Health and Human Services. Public Health Service. Centers for Disease Control. Center for Chronic Disease Prevention and Health Promotion. Office on Smoking and Health. The Health Benefits of Smoking Cessation-a report of the Surgeon General. DHHS Publication No. (CDC) 90-8416. Rockville (MD): CDC; 1990.
60. Chopra GS. Studies on psycho-clinical aspects of long-term marihuana use in 124 cases. Int J Addict. 1973;8(6):1015-26. https://doi.org/10.3109/10826087309033103
61. Chatkin JM, Zani-Silva L, Ferreira I, Zamel N. Cannabis-Associated Asthma and Allergies. Clin Rev Allergy Immunol. 2019;56(2):196-206. https://doi.org/10.1007/s12016-017-8644-1
62. Chatkin JM, Zabert G, Zabert I, Chatkin G, Jiménez-Ruiz CA, de Granda-Orive JI, et al. Lung Disease Associated with Marijuana Use. Arch Bronconeumol. 2017;53(9):510-515. https://doi.org/10.1016/j.arbres.2017.03.019
63. Gaeta TJ, Hammock R, Spevack TA, Brown H, Rhoden K. Association between substance abuse and acute exacerbation of bronchial asthma. Acad Emerg Med. 1996; 3:1170-2. https://doi.org/10.1111/j.1553-2712.1996.tb03386.x
64. Caponnetto P, Auditore R, Russo C, Alamo A, Campagna D, Demma S, et al. "Dangerous relationships": asthma and substance abuse. J Addict Dis. 2013;32(2):158-67. https://doi.org/10.1080/10550887.2013.795469
65. Decuyper II, Faber MA, Sabato V, Bridts CH, Hagendorens MM, Rihs HP, et al. Where there's smoke, there's fire: cannabis allergy through passive exposure. J Allergy Clin Immunol Pract. 2017;5(3):864-865. https://doi.org/10.1016/j.jaip.2016.10.019
66. McLeish AC, Zvolensky MJ. Asthma and cigarette smoking: a review of the empirical literature. J Asthma. 2010;47(4):345-61. https://doi.org/10.3109/02770900903556413
67. Perret JL, Bonevski B, McDonald CF, Abramson MJ. Smoking cessation strategies for patients with asthma: improving patient outcomes. J Asthma Allergy. 2016;9:117-28. https://doi.org/10.2147/JAA.S85615
68. Bush T, Zbikowski SM, Mahoney L, Deprey M, Mowery P, Cerutti B. State quitlines and cessation patterns among adults with selected chronic diseases in 15 states, 2005-2008. Prev Chronic Dis. 2012;9:E163. https://doi.org/10.5888/pcd9.120105
69. McLeish AC, Johnson AL, Avallone KM, Zvolensky MJ. Evaluating the role of anxiety sensitivity in barriers to cessation and reasons for quitting among smokers with asthma. Psychol Health Med. 2016;21(2):236-47. https://doi.org/10.1080/13548506.2015.1051058
70. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Updated 2018. Bethesda: Global Initiative for Chronic Obstructive Lung Disease; 2018.
71. U.S. Department of Health and Human Services. Public Health Service. Office of the Surgeon General [homepage on the Internet]. Rockville (MD): U.S. Department of Health and Human Services The Health Consequences of Smoking: 50 Years of Progress. A Report of the Surgeon General. Atlanta (GA): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014. [Adobe Acrobat document, 1081p.]. Available from: https://www.surgeongeneral.gov/library/reports/50-years-of-progress/full-report.pdf
72. Liu S, Zhou Y, Liu S, Chen X, Zou W, Zhao D, et al. Association between exposure to ambient particulate matter and chronic obstructive pulmonary disease: results from a cross-sectional study in China. Thorax. 2017:72(9):788-795. https://doi.org/10.1136/thoraxjnl-2016-208910
73. Moreira MA, Barbosa MA, Jardim JR, Queiroz MC, Inácio LU. Doença pulmonar obstrutiva crônica em mulheres expostas à fumaça de fogão e lenha. Rev Assoc Med Bras (1992). 2013;59(6):607-13. https://doi.org/10.1016/j.ramb.2013.09.001
74. Sana A, Somda SMA, Meda N, Bouland C. Chronic obstructive pulmonary disease associated with biomass fuel use in women: a systematic review and meta-analysis. BMJ Open Respir Res. 2018;5(1):e000246. https://doi.org/10.1136/bmjresp-2017-000246
75. Bahtt S, Kim Y, Harrington K, Lutz SM, Cho MH, DeMeo DL, et al. Smoking duration alone provides stronger risk estimates of chronic pulmonary obstructive disease than pack-years. Thorax. 2018;73(5):414-421. https://doi.org/10.1136/thoraxjnl-2017-210722
76. Queiroz MC, Moreira MA, Rahabi MF. Underdiagnosis of COPD at primary health care clinics in the city of Aparecida de Goiânia, Brazil. J Bras Pneumol. 2012;38(6):692-9. https://doi.org/10.1590/S1806-37132012000600003
77. Moreira GL, Manzano BM, Gazzotti MR, Nascimento OA, Perez-Padilla R, Menezes AM, et al. PLATINO, a nine-year follow-up study of COPD in the city of São Paulo, Brazil: the problem of underdiagnosis. J Bras Pneumol. 2014;40(1):30-7. https://doi.org/10.1590/S1806-37132014000100005
78. Menezes AM, Perez-Padilla R, Jardim JR, Mui-o A, Lopez MV, Valdivia G, et al. Chronic obstructive disease in five Latin American cities (the PLATINO study): a prevalence study. Lancet. 2005;366(9500):1875-81. https://doi.org/10.1016/S0140-6736(05)67632-5
79. Lundbäck B, Lindberg A, Lindström M, et al. Not 15 but 50% of smokers develop COPD?--Report from the Obstructive Lung Disease in Northern Sweden Studies. Respir Med. 2003;97(2):155-22. https://doi.org/10.1053/rmed.2003.1446
80. Rennard S, Vestbo J. COPD: the dangerous underestimate of 15%. Lancet 2006;367(9518):1216-9. https://doi.org/10.1016/S0140-6736(06)68516-4
81. Corrêa PC, Barreto SM, Passos VM. Smoking-attributable mortality and years of potential life lost in 16 Brazilian capitals, 2003: a prevalence-based study. BMC Public Health. 2009;9:206. https://doi.org/10.1186/1471-2458-9-206
82. de São José BP, Corrêa RA, Malta DC, Passos VMA, França EB, Teixeira RA, et al. Mortality and disability from tobacco-related diseases in Brazil, 1990 to 2015. Rev Bras Epidemiol. 2017;20(Suppl 1):75-89. https://doi.org/10.1590/1980-5497201700050007
83. Stelmach R, Fernandes FL, Carvalho-Pinto RM, Athanazio RA, Rached SZ, Prado GF, et al. Comparison between objective measures of smoking and self-reported smoking status in patients with asthma or COPD: are our patients telling us the truth? J Bras Pneumol. 2015;41(2):124-32. https://doi.org/10.1590/S1806-37132015000004526
84. van Eard EA, van Rossem CR, Spigt MG, Wesseling G, van Schayck OC, Kotz D. Do we need tailored smoking cessation interventions for smokers with COPD? A comparative study of smokers with and without regarding factors associated with tobacco smoking. Respiration. 2015;90(3):211-9. https://doi.org/10.1159/000398816
85. Tøttenborg SS, Thomsen RW, Johnsen SP, Nielsen H, Lange P. Determinants of Smoking Cessation in Patients With COPD Treated in the Outpatient Setting. Chest. 2016;150(3):554-62. https://doi.org/10.1016/j.chest.2016.05.020
86. Schauer GL, Wheaton AG, Malarcher AM Croft JB. Health-care Provider Screening and Advice for Smoking Cessation Among Smokers With and Without COPD: 2009-2010 National Adult Tobacco Survey. Chest. 2016;149(3):676-84 https://doi.org/10.1378/chest.14-2965
87. Martínez-González C, Casanova C, de-Torres JP, Marín JM, de Lucas P, Fuster A, et al. Changes and Clinical Consequences of Smoking Cessation in Patients With COPD: A Prospective Analysis From the CHAIN Cohort. Chest. 2018;154(2):274-285. https://doi.org/10.1016/j.chest.2018.02.007
88. Bai JW, Chen XX, Liu S, Yu L, Xu J. Smoking cessation affects the natural history of COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:3323-3328. https://doi.org/10.2147/COPD.S150243
89. Tønnesen P, Mikkelsen K, Bremann L. Nurse-conducted smoking cessation in patients with COPD using nicotine sublingual tablets and behavioral support. Chest. 2006;130(2):334-42. https://doi.org/10.1378/chest.130.2.334
90. Godtfredsen NS, Vestbo J, Osler M, Prescott E. Risk of hospital admission for COPD following smoking cessation and reduction: a Danish population study. Thorax. 2002;57(11):967-72. https://doi.org/10.1136/thorax.57.11.967
91. Anthonisen NR, Connet J, Murray RP. Smoking and lung function of Lung Health Study participants after 11 years. Am J Respir Crit Care Med. 2002;166(5):675-9. https://doi.org/10.1164/rccm.2112096
92. Anthonisen NR, Skeans MA, Wise RA, Manfreda J, Kanner RE, Connett JE; et al. The effects of a smoking cessation intervention on 14.5-year mortality: a randomized clinical trial. Ann Intern Med. 2005;142(4):233-9. https://doi.org/10.7326/0003-4819-142-4-200502150-00005
93. Drope J, Schluger N, editors [monograph on the Internet]. 6th ed. The Tobacco Atlas. Atlanta: American Cancer Society and Vital Strategies; 2018. [Adobe Acrobat document, 58p.]. Available from: https://tobaccoatlas.org/wp-content/uploads/2018/03/TobaccoAtlas_6thEdition_LoRes_Rev0318.pdf
94. Rodgman A, Perfetti TA. Alphabetical Component Index. In: Rodgman A, Perfetti TA, editors. The Chemical Components of Tobacco and Tobacco Smoke. Boca Raton (FL): CRC Press; 2008. p. 1483-4. https://doi.org/10.1201/97814200788,, , , , 48
95. IARC Worki, n, g Group on the Evalu,, , , , ation of Carcinogenic Risks to Humans. Tobacco smoke and involuntary smoking. IARC Monogr Eval Carcinog Risks Hum. 2004;83:1-1438.
96. Balogh EP, Dresler C, Fleury ME, Gritz ER, Kean TJ, Myers ML, et al. Reducing tobacco-related cancer incidence and mortality: summary of an institute of medicine workshop. Oncologist. 2014;19(1):21-31. https://doi.org/10.1634/theoncologist.2013-0230
97. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. International Agency for Research on Cancer. Personal habits and indoor combustions. Volume 100 E. A review of human carcinogens. IARC Monogr Eval Carcinog Risks Hum. 2012;100(Pt E):1-538.
98. Álvarez FV, Trueba IM, Sanchis JB, López-Rodó LM, Rodríguez Suárez PM, de Cos Escuín JS, et al. Recommendations of the Spanish Society of Pneumology and Thoracic Surgery on the diagnosis and treatment of non-small-cell lung cancer. Arch Bronconeumol. 2016;52 Suppl 1:2-62.
99. Menezes AM, Horta BL, Oliveira AL, Kaufmann RA, Duquia R, Diniz A, , , , , , et al. Attributed risk to smoking for lung cancer, laryngeal cancer and esophageal cancer [Article in Portuguese]. Rev Saude Publica. 2002;36(2):129-34. https://doi.org/10.1590/S0034-89102002000200002
100. Araujo LH, Baldotto C, Castro G Jr, Katz A, Ferreira CG, Mathias C, et al. Lung cancer in Brazil. J Bras Pneumol. 2018;44(1):55-64. https://doi.org/10.1590/s1806-37562017000000135
101. Azevedo E Silva G, de Moura L, Curado MP, Gomes Fda S, Otero U, Rezende LF, et al. The Fraction of Cancer Attributable to Ways of Life, Infections, Occupation, and Environmental Agents in Brazil in 2020. PLoS One. 2016;11(2):e0148761. https://doi.org/10.1371/journal.pone.0148761
102. Parsons A, Daley A, Begh R, Aveyard P. Influence of smoking cessation after diagnosis of early stage lung cancer on prognosis: Systematic review of observational studies with meta-analysis. BMJ. 2010;340:b5569. https://doi.org/10.1136/bmj.b5569
103. Karam-Hage M, Cinciripini PM, Gritz ER. Tobacco use and cessation for cancer survivors: An overview for clinicians. CA Cancer J Clin. 2014;64(4):272-90. https://doi.org/10.3322/caac.21231
104. Sardari Nia P, Weyler J, Colpaert C, Vermeulen P, Van Marck E, Van Schil P. Prognostic value of smoking status in operated non-small cell lung cancer. Lung Cancer. 2005;47(3):351-9. https://doi.org/10.1016/j.lungcan.2004.08.011
105. Cinciripini P. Smoking Cessation in Patients with Cancer: Treatment Advances and the Oncologist's Role. J Natl Canc Netw. 2017;15(5):748-50. https://doi.org/10.6004/jnccn.2017.0091
106. Gritz ER, Toll BA, Warren GW. Tobacco use in the oncology setting: advancing clinical practice and research. [Internet] Cancer Epidemiol Biomarkers Prev. 2014;23(1):3-9. https://doi.org/10.1158/1055-9965.EPI-13-0896
107. American Society of Clinical Oncology [monograph on the Internet]. Tobacco Cessation Guide for Oncology Providers. Alexandria (VI): ASCO; 2012. [Adobe Acrobat document, 36p.]. Available from: https://moqc.org/wp-content/uploads/2017/08/ASCO-_Tobacco-Cessation-Guide-for-Oncology-Providers.pdf
108. Shields PG, Herbst RS, Arenberg D, Benowitz NL, Bierut L, Luckart JB, et al. Smoking Cessation, Version 1.2016, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2016;14(11):1430-1468. https://doi.org/10.6004/jnccn.2016.0152
109. Koshiaris C, Aveyard P, Oke J, Ryan R, Szatkowski L, Stevens R, et al. Smoking cessation and survival in lung, upper aero-digestive tract and bladder cancer: cohort study Br J Cancer. 2017;117(8):1224-1232. https://doi.org/10.1038/bjc.2017.179
110. World Health Organization. Global tuberculosis report 2017. Geneva: World Health Organization; 2017.
111. Brasil. Ministério de Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Panorama da Tuberculose no Brasil: A mortalidade em números. Brasília: Ministério de Saúde; 2016. [Adobe Acrobat document, 128p.]. Available from: http://portalarquivos2.saude.gov.br/images/pdf/2016/outubro/15/panorama_tuberculose_brasil_mortalidade.pdf
112. World Health Organization. Fact Sheets on Tuberculosis. Geneva: World Health Organization; 2017. Available from: http://www.who.int/tb/publications/factsheet_global.pdf?ua=1
113. Webb G. The effect of the inhalation of cigarette smoke on the lungs: A clinical study. Am Rev Tuberc. 1918;2(1):25-7.
114. World Health Organization; International Union Against Tuberculosis and Lung Diseases. A WHO/The Union monograph on TB and tobacco control: joining efforts to control two related global epidemics. Geneva: WHO; 2007.
115. International Union Against Tuberculosis and Lung Diseases. Smoking Cessation and Smoke-free Environments for Tuberculosis Patients. Paris: International Union Against Tuberculosis and Lung Diseases; 2010.
116. Prasad R, Garg R, Singhal S, Dawar R, Agarwal GG. A case-control study of tobacco smoking and tuberculosis in India. Ann Thorac Med. 2009;4(4):208-10. https://doi.org/10.4103/1817-1737.56007
117. Bates MN, Khalakdina A, Pai M, Chang L, Lessa F, Smith KR. Risk of tuberculosis from exposure to tobacco smoke: a systematic review and meta-analysis. Arch Intern Med. 2007;167(4):335-42. https://doi.org/10.1001/archinte.167.4.335
118. Gajalakshmi V, Peto R, Kanaka TS, Jha P. Smoking and mortality from tuberculosis and other diseases in India: retrospective study of 43000 adult male deaths and 35000 controls. Lancet. 2003;362(9383):507-15. https://doi.org/10.1016/S0140-6736(03)14109-8
119. Slama K, Chiang CY, Enarson DA, Hassmiller K, Fanning A, Gupta P, et al. Tobacco and tuberculosis: a qualitative systematic review and meta-analysis. Int J Tuberc Lung Dis. 2007;11(10):1049-61.
120. Narasimhan P, Wood J, Macintyre CR, Mathai D. Risk factors for tuberculosis. Pulm Med. 2013;2013:828939. https://doi.org/10.1155/2013/828939
121. Sopori M. Effects of cigarette smoke on the immune system. Nat Rev Immunol. 2002;2(5):372-7. https://doi.org/10.1038/nri803
122. Wang H. Yu M, Ochani M, Amella CA, Tanovic M, Susarla S, et al. Nicotinic acetylcholine receptor alpha7 subunit is an essential regulator of inflammation. Nature. 2003;421(6921):384-8. https://doi.org/10.1038/nature01339
123. Ernst JD. The immunological life cycle of tuberculosis. Nat Rev Immunol. 2012;12(8):581-91. https://doi.org/10.1038/nri3259
124. Feng Y, Kong Y, Barnes PF, Huang FF, Klucar P, Wang X, et al. Exposure to cigarette smoke inhibits the pulmonary T-cell response to influenza virus and Mycobacterium tuberculosis. Infect Immun. 2011;79(1):229-37. https://doi.org/10.1128/IAI.00709-10
125. Shang S, Ordway D, Henao-Tamayo M, BaiI X, Oberley-Deegan R, Shanley C, et al. Cigarette smoke increases susceptibility to tuberculosis--evidence from in vivo and in vitro models. J Infect Dis. 2011;203(9):1240-8. https://doi.org/10.1093/infdis/jir009
126. Arcavi L, Benowitz NL. Cigarette smoking and infection. Arch Intern Med. 2004;164(20):2206-16. https://doi.org/10.1001/archinte.164.20.2206
127. Tipayamongkholgul M, Podhipak A, Chearskul S, Sunakorn P. Factors associated with the development of tuberculosis in BCG immunized children. Southeast Asian J Trop Med Public Health. 2005;36(1):145-50.
128. Altet-Gomez MN, Alcaide J, Plans P, Taberner JL, Salto E, Folguera LI, et al. Passive smoking and risk of pulmonary tuberculosis in children immediately following infection. A case-control study. Tuber Lung Dis. 1996;77(6):537-44. https://doi.org/10.1016/S0962-8479(96)90052-0
129. Ariyothai N, Podhipak A, Akarasewi P, Tornee S, Smith-Karn S, Thongprathum P. Cigarette smoking and its relation to pulmonary tuberculosis in adults. Southeast Asian J Trop Med Public Health. 2004;35(1):219-27.
130. Altet-Gômez MN, Alcaide J, Godoy P, Romero MA, Hernández del Rey I. Clinical and epidemiological aspects of smoking and tuberculosis: a study of 13,038 cases. Int J Tuberc Lung Dis. 2005;9(4):430-6.
131. Thomas A, Gopi PG, Santha T, Chandrasekaran V, Subramani R, Selvakumar N, et al. Predictors of relapse among pulmonary tuberculosis patients treated in a DOTS programme in South India. Int J Tuberc Lung Dis. 2005;9(5):556-61.
132. d'Arc Lyra Batista J, de Fátima Pessoa Militão de Albuquerque M, de Alencar Ximenes RA, Rodrigues LC. Smoking increases the risk of relapse after successful tuberculosis treatment. Int J Epid 2008;37(4):841-51. https://doi.org/10.1093/ije/dyn113
133. Cailleaux-Cesar M, Loredo C, Lapa e Silva JR, Conde MB. Impact of smoking on sputum culture conversion and pulmonary tuberculosis treatment outcomes in Brazil: a retrospective cohort study. J Bras Pneumol. 2018;44(2):91-105. https://doi.org/10.1590/s1806-37562017000000161
134. Wen CP, Chan TC, Chan HT, Tsai MK, Cheng TY, Tsai SP. The reduction of tuberculosis risks by smoking cessation. BMC Infect Dis. 2010;10:156. https://doi.org/10.1186/1471-2334-10-156
135. GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1345-1422. https://doi.org/10.1016/S0140-6736(17)32366-8
136. Institute for Health Metrics and Evaluation (IHME) [homepage on the Internet]. Seattle (WA): IHME; [cited 2018 Aug 26]. Brazil. [about 13 screens]. Available from: http://www.healthdata.org/brazil
137. Nemmar A, Holme JA, Rosas I, Schwarze PE, Alfaro-Moreno E. Recent Advances in particulate matter and nanoparticle toxicology: a review of the in vivo and in vitro studies. Biomed Res Int. 2013;2013: 279371. https://doi.org/10.1155/2013/279371
138. World Health Organization [homepage on the Internet]. Geneva: WHO; [updated 2018, cited 2016 Jun 1]. Air pollution [about 3 screens]. Available from: http://www.who.int/airpollution/data/en/
139. Pope CA 3rd, Burnett RT, Turner MC, Cohen A, Krewski D, Jerrett M, et al. Lung cancer and cardiovascular disease mortality associated with ambient air pollution and cigarette smoke: shape of the exposure-response relationships. Environ Health Perspect. 2011;119(11):1616-21. https://doi.org/10.1289/ehp.1103639
140. Nishinakagawa T, Senjyu H, Tanaka T, Asai M, Kotaki K, Yano Y, et al. Smoking aggravates the impaired pulmonary function of officially acknowledged female victims of air pollution of 40 years ago. Tohoku J Exp Med. 2014;234(2):151-60. https://doi.org/10.1620/tjem.234.151
141. Tan CE, Glantz SA. Association between smoke-free legislation and hospitalizations for cardiac, cerebrovascular, and respiratory diseases: a meta-analysis. Circulation. 2012;26(8):2177-83. https://doi.org/10.1161/CIRCULATIONAHA.112.121301
142. Thun MJ, Carter BD, Feskanich D, Freedman ND, Prentice R, Lopez AD, Hartge P, Gapstur SM. 50-year trends in smoking-related mortality in the United States. N Engl J Med. 2013;368(4):351-64. https://doi.org/10.1056/NEJMsa1211127
143. Hessel PA, Gamble JF, Nicolich M. Relationship between silicosis and smoking. Scand J Work Environ Health. 2003;29(5):239-36. https://doi.org/10.5271/sjweh.739
144. Tse LA, Yu IT, Qiu H, Leung CC. Joint effects of smoking and silicosis on diseases to the lungs. PLoS One. 2014;9(8):e104494. https://doi.org/10.1371/journal.pone.0104494
145. GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1151-1210. https://doi.org/10.1016/S0140-6736(17)32152-9
146. GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211-1259. https://doi.org/10.1016/S0140-6736(17)32154-2
147. Syamlal G, King BA, Mazurek JM. Tobacco Use Among Working Adults - United States, 2014-2016. MMWR Morb Mortal Wkly Rep. 2017;66(42):1130-1135. https://doi.org/10.15585/mmwr.mm6642a2
148. Qian QZ, Cao XK, Shen FH, Wang Q. Correlations of smoking with cumulative total dust exposure and cumulative abnormal rate of pulmonary function in coal-mine workers. Exp Ther Med. 2016;12(5):2942-2948. https://doi.org/10.3892/etm.2016.3700
149. Unalacak M, Altin R, Kart L, Tor M, Örnek T, Altunel H. Smoking prevalence, behavior and nicotine addiction among coal workers in Zonguldak, Turkey. J Occup Health. 2004;46(4):289-95. https://doi.org/10.1539/joh.46.289
150. Mana-Salicio VA, Botelho C, Silva AM, Salicio MA. Factors associated with alterations in lung function among workers in the ceramics industry [Article in Portuguese]. Cien Saude Colet. 2013;18(5):1353-1360. https://doi.org/10.1590/S1413-81232013000500020
151. Doll R, Peto R. Boreham J, Sutherland I. Mortality in relation to smoking: 50 years' observations on male British doctors. BMJ. 2004;328(7455):1519. https://doi.org/10.1136/bmj.38142.554479.AE
152. Verbiest M, Brakema E, van der Kleij R, Sheals K, Allistone G, Williams S, et al. National guidelines for smoking cessation in primary care: a literature review and evidence analysis. NPJ Prim Care Respir Med. 2017;27(1):2. https://doi.org/10.1038/s41533-016-0004-8
153. Vassallo R. Diffuse lung diseases in cigarette smokers. Semin Respir Crit Care Med. 2012;33(5):533-42. https://doi.org/10.1055/s-0032-1325162
154. Margaritopoulos GA, Harari S, Caminati A, Antoniou KM. Smoking-related idiopathic interstitial pneumonia: A review. Respirology. 2016;21(1):57-64. https://doi.org/10.1111/resp.12576
155. Margaritopoulos GA, Vasarmidi E, Jacob J, Wells AU, Antoniou KM. Smoking and interstitial lung diseases. Eur Respir Rev. 2015;24(137):428-35. https://doi.org/10.1183/16000617.0050-2015
156. Putman RK, Hatabu H, Araki T, Gudmundsson G, Gao W, Nishino M, et al. Association Between Interstitial Lung Abnormalities and All-Cause Mortality. JAMA. 2016;315(7):672-81. https://doi.org/10.1001/jama.2016.0518
157. Sundram FX. Clinical studies of alveolar-capillary permeability using technetium-99m DTPA aerosol. Ann Nucl Med. 1995;9(4):171-8. https://doi.org/10.1007/BF03168397
158. Feldman C, Anderson R. Cigarette smoking and mechanisms of susceptibility to infections of the respiratory tract and other organ systems. J Infect. 2013;67(3):169-84. https://doi.org/10.1016/j.jinf.2013.05.004
159. Bhat TA, Kalathil SG, Bogner PN, Miller A, Lehmann PV, Thatcher TH, et al. Secondhand Smoke Induces Inflammations and Impairs Immunity to Respiratory Infections. J Immunol. 2018;200(8):2927-2940. https://doi.org/10.4049/jimmunol.1701417
160. De P, Farley A, Lindson N, Aveyard P. Systematic review and meta-analysis: influence of smoking cessation on incidence of pneumonia in HIV. BMC Med. 2013;11:15. https://doi.org/10.1186/1741-7015-11-15
161. Feldman S. Varicella-zoster virus pneumonitis. Chest. 1994;106(1 Suppl):22S-27S. https://doi.org/10.1378/chest.106.1_Supplement.22S
162. Murin S, Bilello KM. Respiratory tract Infections: another reason not to smoke. Cleve Clin J Med. 2005;72(10):916-20. https://doi.org/10.3949/ccjm.72.10.916
163. Lipsky BA, Boyco EJ, Inui TS, Koespsell TD. Risk factors for acquiring pneumococcal Infections. Arch Intern Med. 1986;146(11):2179-85. https://doi.org/10.1001/archinte.1986.00360230105016
164. Wewers MD, Diaz PT, Wewers ME, Lowe MP, Nagaraja HN, Clanton TL. Cigarette smoking in HIV infection induces a suppressive inflammatory environment in the lung. Am J Respir Crit Care Med. 1998;158(5 Pt 1):1543-9. https://doi.org/10.1164/ajrccm.158.5.9802035
165. Correa RA, José BPS, Malta DC, Passos VMA, França EB, Teixeira RA, et al. Burden of disease by lower respiratory tract infections in Brazil, 1990 to 2015: estimates of the Global Burden of Disease 2015 study. Rev Bras Epidemiol. 2017;20Suppl 01(Suppl 01):171-181. https://doi.org/10.1590/1980-5497201700050014
166. Bates MN, Khalakdina A, Pai M, Chang L, Lessa F, Smith KR. Risk of tuberculosis from exposure to tobacco smoke: a systematic review and meta-analysis. Arch Intern Med. 2007;167(4):335-42. https://doi.org/10.1001/archinte.167.4.335
167. Barreto RB, Pincelli M, Steinwandter R, Silva AP, Manes J, Steidle LJ. Smoking among patients hospitalized at a university hospital in the south of Brazil: prevalence, degree of nicotine dependence, and motivational stage of change. J Bras Pneumol. 2012 ;38(1):72-80. https://doi.org/10.1590/S1806-37132012000100011
168. Corrêa AP. Prevalência e perfil tabágico de pacientes adultos internados em unidades cirúrgicas de um hospital universitário. [dissertation]. Porto Alegre: Universidade Federal do Rio Grande do Sul; 2014. 86p. Available from: https://www.lume.ufrgs.br/bitstream/handle/10183/98548/000922413.pdf?sequence=1
169. Rigotti NA, Clair C, Munafo MR, Stead LF. Interventions for smoking cessation in hospitalized patients. Cochrane Database Syst Rev. 2007;(3):CD001837. https://doi.org/10.1002/14651858.CD001837.pub2
170. Jiménez-Ruiz CA, de Granda-Orive JI, Solano Reina S, Riesco-Miranda JA, de Higes-Martinez E, Pascual-Lledó JF, et al. Guidelines for the Treatment of Smoking in Hospitalized Patients. Arch Bronconeumol. 2017;53(7):387-394. https://doi.org/10.1016/j.arbr.2017.05.008
171. Rigotti NA, Clair C, Munafò MR, Stead LF. Interventions for smoking cessation in hospitalized patients. Cochrane Database Syst Rev. 2012;(5):CD001837. https://doi.org/10.1002/14651858.CD001837.pub3
172. Garcia T, Andrade SADS, Biral AT, Bertani AL, Caram LMO, Cezare TJ, et al. Evaluation of smoking cessation treatment initiated during hospitalization in patients with heart disease or respiratory disease. J Bras Pneumol. 2018;44(1):42-48. https://doi.org/10.1590/s1806-37562017000000026
173. Jiménez-Ruiz CA, Andreas S, Lewis KE, Tonnesen P, van Schayck CP, Hajek P, et al. Statement on smoking cessation in COPD and other pulmonary diseases and in smokers with comorbidities who find it difficult to quit. Eur Respir J. 2015;46(1):61-79. https://doi.org/10.1183/09031936.00092614
174. Pederson LL, Wanklin JM, Lefcoe NM. The effects of counseling on smoking cessation among patients hospitalized with chronic obstructive pulmonary disease: a randomized clinical trial. Int J Addict. 1991;26(1):107-19. https://doi.org/10.3109/10826089109056242
175. Ladapo JA, Jaffer FA, Weinstein MC, Froelicher ES. Projected cost-effectiveness of smoking cessation interventions in patients hospitalized with myocardial infarction. Arch Intern Med. 2011;171(1):39-45. https://doi.org/10.1001/archinternmed.2010.479
176. Regan S, Reyen M, Richards AE, Lockhart AC, Liebman AK, Rigotti NA. Nicotine replacement therapy use at home after use during a hospitalization. Nicotine Tob Res. 2012;14(7):885-9. https://doi.org/10.1093/ntr/ntr244











 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket