ABSTRACT
Objective: To evaluate the impact of lipoabdominoplasty on diaphragmatic mobility (DM) and lung function in healthy women. Methods: This was a prospective cohort study using high-resolution ultrasound and forced spirometry to assess DM and lung function, respectively, prior to lipoabdominoplasty, as well as on postoperative day (POD) 10 and POD 30. DM was measured under two conditions: during tidal volume breathing and during a VC maneuver. Results: The sample consisted of 20 women, with a mean age of 39.85 ± 7.52 years and a mean body mass index of 26.21 ± 2.0 kg/m2. Comparing the preoperative and postoperative periods, we found that DM and lung function values were significantly lower after lipoabdominoplasty, the mean DM on POD 10 being 17% and 15% lower during tidal volume breathing and during the VC maneuver, respectively, in comparison with the preoperative mean (p = 0.009 and p < 0.001, respectively). In addition, FEV1, FVC, and PEF were significantly lower on POD 10 than in the preoperative period (p = 0.046, p = 0.002, and p < 0.001, respectively), returning to preoperative values by POD 30. Conclusions: Lipoabdominoplasty appears to have negative short-term repercussions for DM and lung function in healthy women. However, lung function and DM are both apparently restored to preoperative conditions by POD 30.
(ClinicalTrials.gov identifier: NCT02762526 [http://www.clinicaltrials.gov/])
Keywords:
Abdominoplasty; Lipectomy; Ultrasonography; Diaphragm/physiology; Diaphragm/physiopathology; Lung/physiology; Lung/physiopathology; Respiratory mechanics; Spirometry; Respiratory function tests.
RESUMO
Objetivo: Avaliar o impacto da lipoabdominoplastia na mobilidade diafragmática (MD) e na função pulmonar de mulheres saudáveis. Métodos: Estudo prospectivo de coorte com ultrassonografia de alta resolução e espirometria forçada para a avaliação da MD e da função pulmonar, respectivamente, antes da lipoabdominoplastia, no 10º dia do pós-operatório e no 30º dia do pós-operatório. A MD foi medida durante a respiração em volume corrente e durante uma manobra de CV. Resultados: A amostra foi composta por 20 mulheres, com média de idade de 39,85 ± 7,52 anos e média de índice de massa corporal de 26,21 ± 2,0 kg/m2. Ao compararmos os períodos pré e pós-operatório, observamos que a MD e a função pulmonar foram significativamente menores após a lipoabdominoplastia; a média de MD no 10º dia do pós-operatório foi 17% menor durante a respiração em volume corrente e 15% menor durante a manobra de CV do que a média pré-operatória (p = 0,009 e p < 0,001, respectivamente). Além disso, o VEF1, a CVF e o PFE foram significativamente menores no 10º dia do pós-operatório que no pré-operatório (p = 0,046, p = 0,002 e p < 0,001, respectivamente), retornando aos valores pré-operatórios até o 30º dia do pós-operatório. Conclusões: A lipoabdominoplastia parece ter repercussões negativas em curto prazo na MD e função pulmonar de mulheres saudáveis. No entanto, tanto a função pulmonar como a MD aparentemente retornam ao estado pré-operatório até o 30º dia do pós-operatório.
(ClinicalTrials.gov identifier: NCT02762526 [http://www.clinicaltrials.gov/])
Palavras-chave:
Abdominoplastia; Lipectomia; Ultrassonografia; Diafragma/fisiologia; Diafragma/fisiopatologia; Pulmão/fisiologia; Pulmão/fisiopatologia; Mecânica respiratória; Espirometria; Testes de Função Respiratória.
INTRODUÇÃODentre os procedimentos cirúrgicos realizados para modelar o abdome, a lipoabdominoplastia é um dos mais solicitados: é a terceira cirurgia plástica mais realizada em todo o mundo.(1-4) Além de resultar em redução significativa do coxim adiposo, a lipoabdominoplastia, uma combinação de abdominoplastia clássica com lipoaspiração, tem outros benefícios: plicatura muscular e remoção de tecido cutâneo.(5) A lipoabdominoplastia tornou-se prática comum entre os cirurgiões plásticos, e a incidência de complicações pós-operatórias é baixa se o estado clínico do paciente é avaliado antes do procedimento.(5,6) No entanto, há relatos de comorbidades respiratórias no pós-operatório da lipoabdominoplastia, tais como insuficiência respiratória, atelectasia, pneumonia e broncoespasmo.(7-11) Essas complicações podem ser atribuídas ao aumento da pressão intra-abdominal (PIA), o qual é causado pela plicatura da aponeurose do músculo reto abdominal e pode resultar em alterações da mobilidade diafragmática (MD)(12) e prejuízo da função pulmonar.(10,13) Em alguns dos casos relatados, a função pulmonar foi reduzida à metade da observada antes da cirurgia. Embora a MD não tenha sido avaliada em nenhum dos relatos supracitados, outros fatores foram implicados na redução pós-operatória dos volumes pulmonares, tais como a administração de anestésicos, a manipulação visceral, a incisão na parede abdominal e o medo que os pacientes têm de lesão decorrente da cirurgia.(6,14) A dor afeta a evolução pós-operatória de pacientes submetidos à cirurgia abdominal, com impacto negativo na função pulmonar.(15)
O principal objetivo deste estudo foi identificar complicações respiratórias em mulheres saudáveis submetidas à lipoabdominoplastia. Para isso, a MD e a função pulmonar foram avaliadas em momentos distintos.
MÉTODOSDesenho e participantes do estudoTrata-se de um estudo prospectivo de coorte realizado entre julho de 2015 e março de 2016 no Setor de Fisioterapia do Laboratório de Fisiologia e Fisioterapia Cardiorrespiratória e na Clínica de Cirurgia Plástica do Hospital das Clínicas da Universidade Federal de Pernambuco (HC-UFPE), bem como na Clínica de Cirurgia Plástica do Hospital Agamenon Magalhães. O estudo foi aprovado pelo Comitê de Ética em Pesquisa com Seres Humanos do Centro de Ciências da Saúde do HC-UFPE (CAAE: 15225913.0.0000.5208) e foi registrado no ClinicalTrials.gov (identificador: NCT02762526). O processo de amostragem empregado foi não probabilístico, no qual foram avaliadas todas as mulheres que preencheram os critérios de elegibilidade.
Critérios de elegibilidadeForam incluídas mulheres entre 25 e 55 anos de idade submetidas à lipoabdominoplastia com plicatura do músculo reto abdominal. Todas apresentavam deformidade abdominal do tipo IV ou V, como descrito por Bozola.(16) Foram selecionadas mulheres sem histórico de comorbidades respiratórias ou cardíacas, com índice de massa corporal ≤ 30 kg/m2 e pelo menos 18 pontos no Miniexame do Estado Mental.
Foram excluídas fumantes atuais e mulheres com carga tabágica maior que 10 anos-maço. Foram também excluídas mulheres com VEF1 < 80% do valor previsto ou relação VEF1/CVF < 70% do valor previsto.
Procedimento cirúrgicoPara o procedimento cirúrgico, todas as pacientes foram sedadas e receberam anestesia raquidiana ou peridural. Primeiro, o sítio cirúrgico foi marcado. Uma solução de adrenalina (em soro fisiológico a 1:250.000) foi então injetada na cavidade abdominal a fim de iniciar a lipoaspiração. A aspiração foi iniciada pela região supraumbilical e prosseguiu pelos lados e região infraumbilical. Após a lipoaspiração, o umbigo foi isolado e apenas a pele infraumbilical foi ressecada, como na abdominoplastia clássica.(5)
A umbilicoplastia foi realizada por meio da fixação da derme profunda do umbigo à aponeurose do músculo reto abdominal; em seguida, a derme profunda do novo umbigo foi fixada ao retalho por meio de sutura com Monocryl® 3-0 nos pontos colaterais. O retalho cutâneo foi fixado em dois planos, com fio mononáilon 3-0 no tecido subcutâneo e Monocryl® 5-0 na derme, inicialmente com pontos simples separados e, em seguida, com sutura contínua. Nos pontos colaterais e cardeais do umbigo, respectivamente, foram usadas a sutura de Allgöwer-Donati modificada e sutura simples, ambos com fio mononáilon 4-0.(17)
Medidas de desfechoTodos os desfechos investigados foram medidos em três momentos: no pré-operatório, no 10º dia do pós-operatório e no 30º dia do pós-operatório. Inicialmente, todas as pacientes foram submetidas a anamnese e exame físico. Além da coleta de dados pessoais, foram registradas as medidas antropométricas - peso (em kg), estatura (em m) e índice de massa corporal (em kg/m2) - e os sinais vitais (FC, SpO2, FR e pressão arterial). As pacientes foram instruídas a permanecer sentadas com os braços sobre as pernas e em silêncio durante a mensuração dos sinais vitais.
MDFoi usado um aparelho de ultrassonografia de alta resolução (SonoAce R3; Samsung Medison, Seul, Coreia do Sul) com um transdutor convexo de 3,5 MHz. O protocolo usado foi o sugerido por Testa et al.(12,18) As pacientes foram instruídas verbalmente a respirar de maneira regular para que a MD fosse medida durante a respiração em volume corrente (VC) e, em seguida, realizar manobras de CV (Figura 1), durante as quais cada curva referente ao deslocamento da cúpula diafragmática (em mm) foi medida imediatamente após a aquisição das imagens. As manobras foram repetidas a fim de obter cinco imagens satisfatórias. Foi considerada a média dos três valores maiores com no máximo 10% de diferença um do outro.
 Função pulmonar
Função pulmonarA fim de avaliar a CVF, o VEF1, o FEF entre 25% e 75% da CVF (FEF25-75%), o PFE e a relação VEF1/CVF, foi usado um espirômetro portátil (Microloop MK8; Micro Medical, Kent, Inglaterra). As manobras foram realizadas em conformidade com as recomendações da American Thoracic Society(19) e outras diretrizes de testes de função pulmonar.(20)
DispneiaOs pacientes responderam a perguntas sobre sua percepção de dispneia em repouso e durante os procedimentos realizados. Foi aplicada a Escala modificada de Borg, em conformidade com as recomendações da American Thoracic Society.(19)
DorFoi usada uma escala visual analógica(21) unidimensional para determinar o grau de intensidade da dor. A dor foi avaliada em repouso durante cada avaliação respiratória. Para evitar um viés de aferição, todos os procedimentos foram realizados pelo mesmo examinador durante todas as fases do estudo.
Análise estatísticaO tamanho da amostra foi calculado por meio do programa G*Power3,(22) com base nos resultados de um estudo piloto com 10 pacientes. O cálculo foi realizado por meio da determinação da média da diferença entre o valor pré-operatório e o valor obtido no 10º dia do pós-operatório (∆1), bem como entre o valor pré-operatório e o valor obtido no 30º dia do pós-operatório (∆2) para as variáveis clinicamente mais relevantes: VEF1, CVF e MD. Para o VEF1, ∆1 foi = 13,4 ± 5 e ∆2 foi = 3,5 ± 3. Para a CVF, ∆1 foi = 11,8 ± 2,62 e ∆2 foi = 4,7 ± 4,5. Para a MD, ∆1 foi = 18 ± 7,16 e ∆2 foi = 2,62 ± 3,13. Portanto, seriam necessários 5 pacientes para o VEF1, 7 para a CVF e 7 para a MD, o que daria a todas essas variáveis um poder de 95% e um alfa de 0,05. No entanto, optou-se por selecionar 27 pacientes, considerando o potencial de perdas de seguimento em estudos prospectivos de coorte.
Os dados foram analisados por meio do programa SigmaPlot para Windows, versão 12.0 (Systat Software, San Jose, CA, EUA). Para caracterizar a amostra, foi realizada uma análise estatística descritiva, com média ± desvio-padrão, média (IC95%) ou mediana (intervalo interquartil) para as variáveis quantitativas.
O teste de Shapiro-Wilk e o teste de Levene para homogeneidade de variância foram aplicados para verificar a normalidade e a homogeneidade dos dados, respectivamente. Para comparar os momentos avaliados, foram usados a ANOVA de duas vias para medidas repetidas e o teste post hoc de Holm-Sidak para comparar as médias das variáveis quantitativas com distribuição homogênea normal. Para as variáveis quantitativas sem distribuição normal, foi usada a ANOVA por postos de Friedman para medidas repetidas e, em seguida, o teste post hoc de Tukey para aquelas que apresentaram diferença estatística. O tamanho do efeito foi determinado pelo cálculo do d de Cohen, que consistiu em obter a média da diferença entre os momentos avaliados e dividir o resultado pelo desvio-padrão combinado.(23) O coeficiente de correlação de Pearson foi usado para detectar relações entre variáveis de MD e de função pulmonar. As análises estatísticas foram realizadas por meio do programa IBM SPSS Statistics, versão 20.0 (IBM Corporation, Armonk, NY, EUA). Valores de p < 0,05 foram considerados estatisticamente significativos.
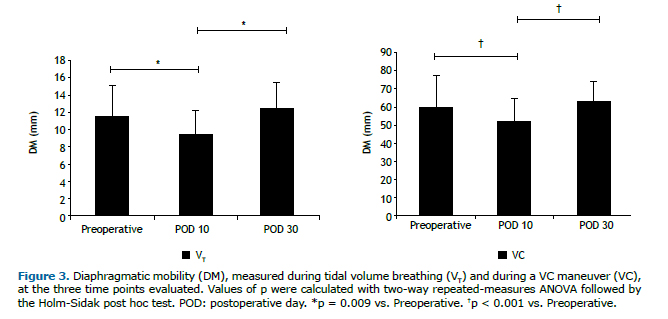
RESULTADOSA amostra inicial foi composta por 27 mulheres, todas as quais foram submetidas à lipoabdominoplastia. No entanto, apenas 20 completaram o protocolo (Figura 2). As variáveis antropométricas, as características clínicas e os sinais vitais são apresentados resumidamente na Tabela 1. Duas pacientes foram excluídas da análise da MD, em virtude de problemas técnicos na ultrassonografia. No 10º dia do pós-operatório, a MD durante a respiração em VC e na CPT foi relativamente baixa (9,54 mm (8,42-10,99 mm) e 51,23 mm (41,66-55,89 mm), respectivamente), mas voltou ao normal até o 30º dia do pós-operatório (12,37 mm (10,49-14,13 mm) e 63,35 mm (55,19-68,34 mm), respectivamente), quando se mostrou comparável à observada no pré-operatório (11,56 mm (9,65-13,48 mm) e 60,15 mm (51,95-67,84 mm), respectivamente). Como se pode observar na Figura 3, as diferenças entre os valores pré e pós-operatórios foram significativas no que tange às imagens adquiridas durante a respiração em VC (p = 0,009) e àquelas adquiridas durante a manobra de CV (p < 0,001).


Os parâmetros de função pulmonar nos três momentos avaliados são apresentados na Tabela 2. Houve diferenças significativas entre os momentos quanto ao VEF1, CVF e PFE, todos os quais foram menores no 10º dia do pós-operatório que no pré-operatório e retornaram ao normal até o 30º dia do pós-operatório. A relação VEF1/CVF e o FEF25-75% permaneceram inalterados após a lipoabdominoplastia, sem diferenças estatísticas entre os momentos avaliados. No 10º dia do pós-operatório, a MD medida durante a manobra de CV correlacionou-se positivamente, embora moderadamente, com o VEF1 (r = 0,502; p = 0,034) e o PFE (r = 0,515; p = 0,029), como se pode observar na Figura 4.


Das 20 mulheres avaliadas, 7 relataram dor no 10º dia do pós-operatório. Três delas consideraram sua dor leve e 4 a consideraram moderada. Uma das mulheres relatou dor moderada no 30° dia do pós-operatório. Duas mulheres relataram sensação de dispneia no 10º dia do pós-operatório: em uma delas, a dispneia foi considerada não muito intensa e, na outra, foi considerada muito intensa. No 30º dia do pós-operatório, nenhuma das pacientes relatou dispneia. Não foram observadas diferenças entre os relatos de dor/dispneia em repouso e os de dor/dispneia durante a execução das manobras, nem no tocante à percepção ou intensidade da dor nem no tocante à percepção de dispneia, em nenhum dos momentos avaliados.
DISCUSSÃOOs principais achados de nosso estudo são que a lipoabdominoplastia com plicatura do músculo reto abdominal promoveu redução da MD e piora da função pulmonar em mulheres saudáveis, conforme a avaliação realizada no 10º dia do pós-operatório. No entanto, ambos os parâmetros tenderam a retornar aos valores pré-operatórios até o 30º dia do pós-operatório.
Em comparação com as médias pré-operatórias, a média da MD no 10º dia do pós-operatório foi 17% menor quando medida durante a respiração em VC e 15% menor quando medida durante a manobra de CV. Até o 30º dia do pós-operatório, a MD havia retornado a valores comparáveis aos obtidos no período pré-operatório. No entanto, há poucos estudos nos quais a MD é avaliada nessa população específica, o que impossibilita qualquer comparação com nossos achados.
Supomos que haja dois grandes motivos pelos quais a MD em nossa amostra tenha se comportado como se comportou. O primeiro deles é a influência da plicatura do músculo reto abdominal próximo ao apêndice xifoide, e o segundo é o aumento da PIA.
No que tange à influência da plicatura do músculo reto abdominal, nossa hipótese é a de que a aproximação das bordas do músculo possa gerar maior resistência à tração em suas fibras, reduzindo o diâmetro anteroposterior e o diâmetro transverso do tórax, o que por sua vez reduz a MD, em virtude da proximidade anatômica entre as inserções superiores do músculo reto abdominal e uma das origens do diafragma. O músculo reto abdominal se liga à quinta, sexta e sétima cartilagem costal e ao apêndice xifoide, ao passo que a porção costal do diafragma é também oriunda das últimas seis costelas. Além disso, a postura de flexão do tronco adotada pelo paciente durante pouco mais de 10 dias depois do procedimento pode aumentar a magnitude das alterações.(24,25)
A principal função do músculo transverso abdominal e do músculo oblíquo abdominal é puxar a parede abdominal para dentro, aumentando a PIA. Ao fazê-lo, esses músculos induzem o deslocamento cranial do diafragma, o que resulta em aumento da pressão pleural e, consequentemente, redução do volume pulmonar. Embora o músculo reto abdominal tenha que fazer o mesmo quando a parede abdominal ventral apresenta convexidade externa, seria de se esperar que, quando a convexidade fosse interna, uma contração muscular isolada puxasse a parede levemente para fora.(26) Em um estudo com animais, De Troyer et al.(27) analisaram a ativação seletiva do músculo reto abdominal por estimulação elétrica e constataram que a caixa torácica e o esterno foram deslocados na direção caudal e anteroposterior, ao passo que os diâmetros transversos da caixa torácica inferior diminuíram. Portanto, a plicatura do músculo reto abdominal resulta em aumento da PIA e da pressão pleural, independentemente da forma da parede abdominal. Apesar das limitações da comparação, esses achados corroboram a hipótese aventada em nosso estudo: a de que a plicatura da aponeurose gera tensão e, assim, limita a expansão torácica. Nossa hipótese é a de que a redução da MD também pode ser explicada pelo aumento pós-operatório da PIA - que persistiu até o 10º dia do pós-operatório, no mínimo - causado pela plicatura do músculo reto abdominal para correção de diástase, que impede a descida do diafragma.(26) Após a plicatura, a região abdominal pode auxiliar adequadamente na expansão pulmonar e a PIA permanece normal (isto é, ≤ 5 mmHg em adultos saudáveis). Pressões acima de 15 mmHg podem causar mais danos ao sistema respiratório.(28,29) Embora nosso estudo não apresente a PIA das mulheres submetidas à lipoabdominoplastia, outros autores descreveram o comportamento da PIA após procedimentos cirúrgicos semelhantes. Talisman et al.(30) mediram as oscilações da PIA durante a abdominoplastia em 18 pacientes e estudaram a relevância dessas oscilações para a evolução de pacientes no pós-operatório imediato. Três pacientes submetidos à plicatura para correção de diástase do músculo reto abdominal apresentaram PIA acima de 24 cmH2O no pós-operatório imediato e acima de 20 cmH2O no 1º dia do pós-operatório. Os autores concluíram que o risco de apresentar desconforto respiratório no pós-operatório imediato é maior em tais pacientes.
A plicatura do músculo reto abdominal próximo ao apêndice xifoide e o consequente aumento da PIA resultam em desvantagem mecânica para o diafragma, o que resulta em distúrbio ventilatório restritivo em pacientes submetidos a esse tipo de cirurgia. Nas pacientes que fizeram parte de nossa amostra, observamos uma redução dos parâmetros espirométricos no pós-operatório, e esses valores mais baixos persistiram até o 10° dia do pós-operatório, no mínimo.
Os dados espirométricos obtidos em nosso estudo mostram que houve grande piora da função pulmonar no 10º dia do pós-operatório, com redução do VEF1 e da CVF, e quase completo restabelecimento da função pulmonar normal até o 30º dia do pós-operatório. Da mesma forma, o PFE mostrou-se diminuído no 10º dia do pós-operatório e retornou aos valores pré-operatórios no 30º dia do pós-operatório, com diferença significativa entre o 10º e o 30º dia do pós-operatório. Durante o estudo, não houve alterações significativas do FEF25-75% ou da relação VEF1/CVF. Esses dados sugerem que a lipoabdominoplastia contribui para o surgimento de distúrbio ventilatório restritivo.
Pelo que sabemos, nenhum outro estudo avaliou a função pulmonar em mulheres submetidas à lipoabdominoplastia. No entanto, outros autores estudaram o comportamento da função pulmonar no pós-operatório de abdominoplastia e observaram que a função pulmonar piora no pós-operatório imediato e retorna ao estado pré-operatório até o 30º dia do pós-operatório.(10,13,31,32) Optamos por avaliar as pacientes nesse momento com base nesses estudos. Tercan et al.(10) avaliaram 14 mulheres saudáveis submetidas à abdominoplastia e observaram uma diminuição significativa da CVF no 10º dia do pós-operatório, que melhorou até o 30º dia do pós-operatório, quando a CVF superou a observada no pré-operatório, o que sugere que a correção da diástase do músculo reto abdominal é eficaz em conter a parede abdominal, melhorando os parâmetros espirométricos ao longo de um período > 30 dias. Da mesma forma, Helene Junior et al.(13) observaram que, em pacientes submetidos à abdominoplastia, o VEF1, a CVF, o FEF25-75% e o PFE foram menores no 4º dia do pós-operatório que no período pré-operatório, com relação VEF1/CVF constante não obstante o VEF1 e a CVF abaixo do normal, sugerindo a presença de padrão restritivo. Os autores observaram também que a CVF e o PFE melhoraram significativamente do 4º para o 15º dia do pós-operatório, bem como do 15º para o 30º dia do pós-operatório, embora nem a CVF nem o PFE tenham retornado aos valores pré-operatórios. Em um estudo em longo prazo com 24 pacientes submetidos à abdominoplastia completa, Perin et al.(31) avaliaram os parâmetros espirométricos durante o pré-operatório e após uma média de 28 meses. Os autores não observaram nenhuma diferença entre esses dois momentos no que tange à função pulmonar dos pacientes. Rodrigues et al.(32) estudaram a função respiratória de pacientes submetidos a plicatura da aponeurose do músculo oblíquo abdominal externo e correção de diástase do músculo reto abdominal. Os autores observaram um padrão ventilatório semelhante ao que ocorre no pós-operatório em pacientes submetidos apenas a correção de diástase do músculo reto abdominal e concluíram que a plicatura em forma de L, por si só, não aumenta a PIA, isto é, ela não é responsável pelo comprometimento da função pulmonar após a abdominoplastia. Os autores atribuíram o significativo aumento da PIA no pós-operatório ao uso de uma roupa de compressão, considerado pelos autores o fator mais prejudicial.
No presente estudo, notamos que, no 10º dia do pós-operatório, a MD durante a manobra de CV correlacionou-se com a função pulmonar. Buscamos correlações nesse momento porque acreditamos que as limitações em pacientes submetidos à lipoabdominoplastia são maiores nos 10 primeiros dias após o procedimento. Nas pacientes que compuseram nossa amostra, a MD durante a manobra de CV apresentou moderada correlação positiva com o PFE e com o VEF1, embora a MD durante a respiração em VC não tenha se correlacionado com nenhum dos parâmetros espirométricos. Esses dados indicam que algumas das limitações da função pulmonar nessas pacientes podem ser explicadas pela redução da MD causada pela plicatura, sendo que essa redução é mais pronunciada durante o esforço máximo, já que a amostra foi composta por mulheres saudáveis. Provavelmente haveria forte correlação entre função pulmonar e MD, inclusive entre função pulmonar e MD durante a respiração em VC, em uma população com comorbidades pré-existentes.
Em nosso estudo, a dor, medida por meio de uma escala visual analógica, foi relatada por 35% e 5% das pacientes no 10º e no 30º dia do pós-operatório, respectivamente. Embora alguns estudos tenham mostrado que a dor pós-operatória pode estar relacionada com redução dos volumes pulmonares,(33) não observamos nenhuma correlação entre dor e função pulmonar. Também não consideramos a dor um fator relevante para a disfunção diafragmática, pois o comportamento dos parâmetros espirométricos e da MD nas pacientes com dor foi semelhante ao observado naquelas sem dor. É possível que isso tenha ocorrido em virtude do fato de que apenas 7 mulheres relataram dor, provavelmente porque a maioria das pacientes recebeu analgésicos, prática comum no período pós-operatório. Além disso, diferentemente do que ocorre durante a cirurgia abdominal alta, não ocorre ruptura de fibras musculares durante a lipoabdominoplastia, o que é uma distinção importante, pois a lesão muscular é a principal causa de dor pós-operatória.(34)
No 10º dia do pós-operatório, as pacientes que compuseram nossa amostra apresentaram redução da MD e da função pulmonar. No entanto, a dispneia não foi um fator clínico importante em nosso estudo: ela foi relatada por apenas 10% das pacientes avaliadas.
Nosso estudo apresenta algumas limitações, tais como o fato de que não avaliamos nem a força muscular respiratória nem a espessura do diafragma. São, portanto, necessários mais estudos, nos quais se avaliem a força muscular respiratória e a espessura do diafragma, para elucidar nossos achados.
REFERÊNCIAS1. Santos NP Dos, Barnabé AS, Fornari JV, Ferraz RRN. Pain assessment in patients undergoing cosmetic or reconstructive plastic surgery [Article in Portuguese]. Rev Bras Cir Plast. 2012;27(2):190-4.
2. American Society of Plastic Surgeons [homepage on the Internet]. Arlington Heights (IL): the Society; c2008 [cited 2017 Nov 1]. Report of the 2007 statistics: National Clearinghouse of Plastic Surgery Statistics. Available from: www.plasticsurgery.org/
3. Rohrich RJ, Stuzin JM. Globalization of plastic surgery: the world of plastic and reconstructive surgery in Brazil. Plast Reconstr Surg. 2012;130(4):967-8. https://doi.org/10.1097/PRS.0b013e31826703b1
4. Nahas FX. A pragmatic way to treat abdominal deformities based on skin and subcutaneous excess. Aesthetic Plast Surg. 2001;25(5):365-71. https://doi.org/10.1007/s00266-001-0025-7
5. Saldanha OR, Pinto EBS, Matos Jr WN, Lucon RL, Magalhães F, Bello EML, et al. Lipoabdominoplasty - Saldanha's Technique. Rev Bras Cir Plast. 2003;(2):37-46.
6. Assumpção GG. Mini-abdominoplasty associated with liposuction and lowering of the umbilical scar without pedicular detachment [Article in Portuguese]. Rev Bras Cir Plast. 2012;27(3):450-6. https://doi.org/10.1590/S1983-51752012000300021
7. ROE BB. Prevention and treatment of respiratory complications in surgery. N Engl J Med. 1960;263:547-50. https://doi.org/10.1056/NEJM196009152631106
8. Palmon SC, Kirsch JR, Depper JA, Toung TJ. The effect of the prone position on pulmonary mechanics is frame-dependent. Anesth Analg. 1998;87(5):1175-80.
9. Rezaiguia S, Jayr C. Prevention of respiratory complications after abdominal surgery [Article in French]. Ann Fr Anesth Reanim. 1996;15(5):623-46. https://doi.org/10.1016/0750-7658(96)82128-9
10. Tercan M, Bekerecioglu M, Dikensoy O, Kocoglu H, Atik B, Isik D, et al. Effects of abdominoplasty on respiratory functions: a prospective study. Ann Plast Surg. 2002;49(6):617-20. https://doi.org/10.1097/00000637-200212000-00011
11. Pierri A, Munegato G, Carraro L, Zaccaria F, Tiso E, Zotti EF. Hemodynamic alterations during massive incisional hernioplasty. J Am Coll Surg. 1995;181(4):299-302.
12. Yamaguti WP, Paulin E, Shibao S, Kodaira S, Chammas MC, Carvalho CR. Ultrasound evaluation of diaphragmatic mobility in different postures in healthy subjects. J Bras Pneumol. 2007;33(4):407-13. https://doi.org/10.1590/S1806-37132007000400009
13. Helene Junior A, Saad Junior R, Stirbulov R. Avaliação da função respiratória em indivíduos submetidos à abdominoplastia. Rev Col Bras Cir. 2006;33(1):45-50. https://doi.org/10.1590/S0100-69912006000100011
14. Grams ST, von Saltiél R, Mayer AF, Schivinski CI, de S Nobre LF, Nóbrega IS, et al. Assessment of the reproducibility of the indirect ultrasound method of measuring diaphragm mobility. Clin Physiol Funct Imaging. 2014;34(1):18-25. https://doi.org/10.1111/cpf.12058
15. Tonella RM, Araújo S, Silva AM. Transcutaneous electrical nerve stimulation in the relief of pain related to physical therapy after abdominal surgery [Article in Portuguese]. Rev Bras Anestesiol. 2006;56(6):630-42.
16. Bozola AR. Abdominoplasty: same classification and a new treatment concept 20 years later. Aesthetic Plast Surg. 2010;34(2):181-92. https://doi.org/10.1007/s00266-009-9407-z
17. Pigossi N, Tariki JY, de Cássia H, Calonge F, de Andrade AC, Misawa HT, et al. Tactics in the umbilical approach in abdominoplasties [Article in Portuguese]. Rev Hosp Clin Fac Med Sao Paulo. 1991;46(3):145-7.
18. Testa A, Soldati G, Giannuzzi R, Berardi S, Portale G, Gentiloni Silveri N. Ultrasound M-mode assessment of diaphragmatic kinetics by anterior transverse scanning in healthy subjects. Ultrasound Med Biol. 2011;37(1):44-52. https://doi.org/10.1016/j.ultrasmedbio.2010.10.004
19. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111-7. Erratum in: Am J Respir Crit Care Med. 2016;193(10):1185. https://doi.org/10.1164/ajrccm.166.1.at1102
20. Duarte AA, Pereira CA, Rodrigues SC. Validation of new brazilian predicted values for forced spirometry in caucasians and comparison with predicted values obtained using other reference equations. J Bras Pneumol. 2007;33(5):527-35. https://doi.org/10.1590/S1806-37132007000500007
21. Price DD, McGrath PA, Rafii A, Buckingham B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain. 1983;17(1):45-56. https://doi.org/10.1016/0304-3959(83)90126-4
22. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175-91. https://doi.org/10.3758/BF03193146
23. Sullivan GM, Feinn R. Using Effect Size-or Why the P Value Is Not Enough. J Grad Med Educ. 2012;4(3):279-82. https://doi.org/10.4300/JGME-D-12-00156.1
24. De Troyer A, Estenne M. Functional anatomy of the respiratory muscles. Clin Chest Med. 1988;9(2):175-93.
25. Sieck GC. Diaphragm muscle: structural and functional organization. Clin Chest Med. 1988;9(2):195-210.
26. De Troyer A, Boriek AM. Mechanics of the respiratory muscles. Compr Physiol. 2011;1(3):1273-300. https://doi.org/10.1002/cphy.c100009
27. De Troyer A, Sampson M, Sigrist S, Kelly S. How the abdominal muscles act on the rib cage. J Appl Physiol Respir Environ Exerc Physiol. 1983;54(2):465-9. https://doi.org/10.1152/jappl.1983.54.2.465
28. Luckianow GM, Ellis M, Governale D, Kaplan LJ. Abdominal compartment syndrome: risk factors, diagnosis, and current therapy. Crit Care Res Pract. 2012;2012:908169. https://doi.org/10.1155/2012/908169
29. Sánchez-Miralles A, Castellanos G, Badenes R, Conejero R. Abdominal compartment syndrome and acute intestinal distress syndrome [Article in Spanish]. Med Intensiva. 2013;37(2):99-109. https://doi.org/10.1016/j.medin.2011.11.019
30. Talisman R, Kaplan B, Haik J, Aronov S, Shraga A, Orenstein A. Measuring alterations in intra-abdominal pressure during abdominoplasty as a predictive value for possible postoperative complications. Aesthetic Plast Surg. 2002;26(3):189-92. https://doi.org/10.1007/s00266-001-1469-5
31. Perin LF, Saad R Jr, Stirbulov R, Helene A Jr. Spirometric evaluation in individuals undergoing abdominoplasty. J Plast Reconstr Aesthet Surg. 2008;61(11):1392-4. https://doi.org/10.1016/j.bjps.2008.02.028
32. Rodrigues MA, Nahas FX, Gomes HC, Ferreira LM. Ventilatory function and intra-abdominal pressure in patients who underwent abdominoplasty with plication of the external oblique aponeurosis. Aesthetic Plast Surg. 2013;37(5):993-9. https://doi.org/10.1007/s00266-013-0158-5
33. Nozawa E, Kobayashi E, Matsumoto ME, Feltrim MIZ, Carmona MJC, Auler Júnior JOC. Identificação dos fatores de risco que influenciam no desmame de ventilação mecânica em pacientes traqueostomizados após cirurgia cardíaca. Arq Bras Cardiol. 2003;80(3):301-5.
34. Rodrigues AJ, Évora PRB, Vilela V, Vicente W. Postoperative respiratory complications [Article in Portuguese]. Medicina (Ribeirao Preto). 2008;41(4):469-76. https://doi.org/10.11606/issn.2176-7262.v41i4p469-476











 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket