CENÁRIO PRÁTICOUm grupo de pesquisadores fez um estudo para determinar o grau de acurácia dos níveis séricos de procalcitonina para diagnosticar derrame pleural parapneumônico (DPP) e diferenciá-lo de outras causas de derrame pleural. Eles observaram que a procalcitonina apresentou valor preditivo positivo (VPP) de 66% e valor preditivo negativo (VPN) de 91%.(1)
VPP E VPN DOS TESTES DIAGNÓSTICOSNo artigo anterior,(2) discutimos duas características comuns dos testes diagnósticos, sensibilidade e especificidade, que são características importantes que descrevem a acurácia de um teste. Neste artigo, vamos nos concentrar em aspectos importantes de um teste diagnóstico que nos ajudam a compreender o quão bem um novo teste é capaz de diagnosticar uma doença com base nos resultados do padrão ouro: o VPP e o VPN.
O VPP de um teste diagnóstico é a proporção de indivíduos que apresentam resultado positivo no novo teste e têm a doença segundo o padrão ouro (a proporção de verdadeiro positivos). Quando um teste diagnóstico tem VPP alto, um paciente cujo teste apresente resultado positivo muito provavelmente tem a doença que está sendo investigada.
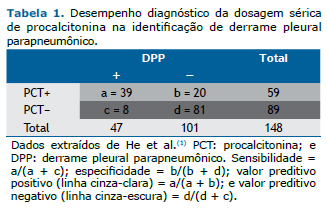
O VPN de um teste diagnóstico é a proporção de indivíduos que apresentam resultado negativo no novo teste e não têm a doença segundo o padrão ouro (a proporção de verdadeiro negativos). Quando um teste tem VPN alto, um paciente cujo teste apresente resultado negativo muito provavelmente não tem a doença que está sendo investigada. Em nosso exemplo, o VPP foi de 66% (39/59) e o VPN foi de 91% (81/89), segundo os resultados do novo teste em 148 indivíduos (Tabela 1).
O VPP e o VPN de um novo teste dependem da prevalência da doença na população; assim, eles serão diferentes em populações com maior ou menor prevalência da doença em comparação com a população na qual o teste foi descrito pela primeira vez. Se a prevalência da doença for alta em uma determinada população, o VPP aumenta e o VPN diminui. Portanto, valores preditivos não são características fixas do teste e não podem ser generalizados para populações com diferentes prevalências da doença.(3) Existe uma maneira fácil de calcular o VPP e o VPN, com base no teorema de Bayes, usando resultados relatados anteriormente e levando em conta a prevalência local da doença.(2)
O VPP e o VPN também são indicadores importantes quando se avalia a população geral. Um teste de rastreamento com alta sensibilidade e especificidade pode ter VPP baixo se a prevalência da doença for baixa nessa população. Por exemplo, quando rastreamos a presença de câncer em adultos assintomáticos, se o VPN do teste for alto, resultados negativos são úteis para descartar a presença da doença; no entanto, se o VPP for baixo, um resultado positivo tem maior probabilidade de ser um falso positivo.
O VPP e o VPN são mais úteis que a sensibilidade e a especificidade para os clínicos porque estimam a probabilidade de doença (ou sua ausência) a partir do resultado do teste. Na próxima e última parte desta série sobre testes diagnósticos, discutiremos razões de verossimilhança e curvas ROC.
REFERÊNCIAS1. He C, Wang B, Li D, Xu H, Shen Y. Performance of procalcitonin in diagnosing parapneumonic pleural effusions: A clinical study and meta-analysis. Medicine (Baltimore). 2017;96(33):e7829. https://doi.org/10.1097/MD.0000000000007829
2. Ferreira JC, Patino CM. Understanding diagnostic tests. Part 1. J Bras Pneumol. 2017;43(5):330. https://doi.org/10.1590/S1806-37562017000000330
3. Altman DG, Bland M. Diagnostic tests. 2: predictive values. BMJ. 1994;309(6947):102. https://doi.org/10.1136/bmj.309.6947.102












 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket