ABSTRACT
Objective: This case study, conducted in the state of Rio Grande do Sul (RS), Brazil, aims to determine the local profile of sarcoidosis, describing patient characteristics, clinical presentation and pulmonary function, as well as analyzing the results of radiological, histopathological and biochemical tests, at the time of diagnosis in a series of sarcoidosis patients. Methods: A retrospective study of 92 patients with sarcoidosis treated on the Pavilhão Pereira Filho (Pereira Filho [Respiratory Diseases] Ward) of the Hospital Santa Casa, in the city of Porto Alegre, RS, between 1990 and 2003. The protocol included the collection of clinical, biochemical, radiological, spirometric and histological data. Results: There was no significant gender-based difference in frequency (men, 42%; women, 58%). Mean age was 41.8 ± 14.1 years, with 87% of patients being between 20 and 60 years old. Caucasians predominated (84%). Most patients (61%) had never smoked, 29% were former smokers, and 10% were current smokers. The majority (33%) of the diagnoses were made in winter. Among the clinical findings, it is of note that 12% were asymptomatic, 18% presented pulmonary symptoms only, 22% presented extrapulmonary symptoms only, and 48% presented pulmonary and extrapulmonary symptoms. Spirometry was performed in 79% of patients at the time of diagnosis. In 45% of those patients, abnormal results were obtained: a restrictive pattern was seen in 23%, an obstructive pattern in 18% and a mixed pattern in 4%. Classification by radiological type revealed that 30% were stage I, 48% were stage II, and 22% were stage III. Conclusion: The findings of this study are quite similar to those of other studies in the literature, particularly those conducted in Europe.
Keywords:
Sarcoidosis, pulmonary/diagnosis; Sarcoidosis, pulmonary/pathology; Lung diseases/pathology; Prognosis; Retrospective studies
RESUMO
Objetivo: Este estudo de casos do Rio Grande do Sul, Brasil, propõe-se a traçar um perfil local da sarcoidose, descrevendo as características dos pacientes, apresentação clínica, função pulmonar, achados radiológicos, histopatológicos e exames bioquímicos de uma série de casos, por ocasião do diagnóstico. Métodos: Estudo retrospectivo de 92 pacientes com sarcoidose, atendidos no Pavilhão Pereira Filho, da Santa Casa de Porto Alegre (RS), entre 1990 e 2003. O protocolo incluiu dados clínicos, bioquímicos, radiológicos, espirométricos e de biópsia. Resultados: Não houve diferença de freqüência entre homens e mulheres (42% e 58%, respectivamente). A média de idade foi de 41,8 ± 14,1 anos, situando-se 87% dos pacientes entre 20 e 60 anos. Houve predomínio em caucasianos (84%). Dados sobre tabagismo mostraram que 61% dos pacientes nunca fumaram, 29% eram ex-fumantes, e 10% ainda fumavam. O diagnóstico foi feito principalmente no inverno (33%). Dentre os dados clínicos destacaram-se: 12% eram assintomáticos, 18% tinham somente sintomas torácicos, 22% somente manifestações extratorácicas, e 48% apresentaram combinação de sintomas torácicos e extratorácicos. A espirometria foi realizada em 79% dos pacientes, no momento do diagnóstico, com resultados anormais em 45% deles, com os seguintes padrões: restritivo em 23%, obstrutivo em 18%, e misto em 4% deles. A distribuição dos tipos radiológicos mostrou 30% tipo I, 48% tipo II e 22% tipo III. Conclusão: Os achados desta série mostraram-se semelhantes aos descritos na literatura, particularmente na européia.
Palavras-chave:
Sarcoidose pulmonar/diagnóstico; Sarcoidose pulmonar/patologia; Pneumopatias/patologia; Prognóstico; Estudos retrospectivos
INTRODUÇÃOA sarcoidose é uma doença granulomatosa, multissistêmica, de causa desconhecida, com atividade imunocelular aumentada, particularmente de células CD4 e macrófagos.(1-6) Embora possa afetar qualquer setor do organismo, pulmões e gânglios intratorácicos são os locais preferidos, ocorrendo em mais de 90% dos casos.(7-8) Mecanismos imunes são importantes na patogenia, presumindo-se que diversos gatilhos possam desencadear a cascata de eventos imunológicos e inflamatórios que caracterizam a doença.(9) Fatores genéticos e raciais também podem determinar maior suscetibilidade à sarcoidose.
Várias avaliações epidemiológicas realizadas em diferentes regiões demonstraram diferenças consideráveis na prevalência, sazonalidade e apresentação clínica da sarcoidose.(10-19) A doença costuma acometer jovens, entre 20 e 40 anos, ocorrendo igualmente tanto em homens quanto em mulheres.(20)
O envolvimento sistêmico da sarcoidose e o achado de alterações em diversos órgãos variam conforme as regiões e as características dos centros de referência.
O diagnóstico de sarcoidose é de exclusão e depende de um conjunto de achados clínicos, radiológicos e laboratoriais. O achado radiológico de adenopatias hilares bilaterais em paciente assintomático é altamente sugestivo de sarcoidose.(21)
O achado histopatológico básico é o de granuloma não caseoso, sem necrose, bem-formado, com abundantes células epitelióides e gigantócitos multinucleados, circundado por anel de linfócitos. Sempre se deve considerar no diagnóstico diferencial doenças granulomatosas de causa conhecida e alta prevalência em nosso meio, como a tuberculose e micoses sistêmicas.(20, 22-24)
O tratamento da sarcoidose visa ao controle dos sintomas, recuperação funcional e regressão das lesões. Como regra, pacientes assintomáticos devem ser observados e não requerem tratamento. O uso de corticóide sistêmico tem se firmado nas últimas décadas como a melhor terapia tanto para pacientes com doença crônica quanto para os períodos de exacerbação.(6,25-26)
Quanto ao prognóstico da sarcoidose, costuma-se referir que, como regra, tem caráter auto-remissivo, evoluindo para a cura, sendo indicadores favoráveis a ela o tipo radiológico I ou um quadro clínico-radiológico agudo ou subagudo associado aos tipos I e II. Apontam para um mau prognóstico a presença do tipo radiológico III, um quadro clínico-radiológico crônico e anormalidades espirométricas, particularmente uma capacidade vital abaixo de 1,5 litros. A mortalidade por sarcoidose é um evento raro e ocorre pela falência de órgãos vitais, devida à fibrose irreversível.(27-28)
As sociedades internacionais publicaram consensos em 1999 que servem como subsídio aos interessados nesta doença.(1-2)
No Brasil, não existem publicações recentes relatando grandes séries de casos de sarcoidose, fato que serviu também como mais um estímulo para este estudo, cujo objetivo é avaliar os dados apresentados por um grupo de pacientes com diagnóstico de sarcoidose e procurar estabelecer um perfil de comportamento da doença em nosso meio. Para tanto, foram levantados dados que caracterizam os pacientes com sarcoidose, bem como suas manifestações clínicas, procedimentos diagnósticos e tratamento.
MÉTODOSEste é um estudo retrospectivo, transversal, que foi realizado no Pavilhão Pereira Filho do Serviço de Pneumologia, Cirurgia Torácica e Radiodiagnóstico do Complexo Hospitalar da Santa Casa de Porto Alegre, um hospital universitário, com execução aprovada pelo comitê de ética em pesquisa da instituição.
Foram encontrados no registro hospitalar 123 pacientes com diagnóstico de sarcoidose, entre os anos de 1990 e 2003, e foram selecionados 92 casos que preencheram os seguintes critérios de inclusão: quadro clínico-radiológico sugestivo ou pelo menos compatível com sarcoidose e material de bió-psia demonstrando granuloma compatível com a doença. Foram excluídos todos os casos em que se constatou extravio de conteúdo do prontuário.
Buscaram-se os seguintes dados: idade, sexo, cor, data do diagnóstico, sintomas torácicos e sistêmicos, sua duração até a primeira consulta, achados radiológicos, calciúria de 24 horas, espirometria, espécime para diagnóstico histológico, alterações extratorácicas e tratamento. Utiliza-se no serviço um protocolo de avaliação inicial para sarcoidose que inclui, necessariamente, os dados acima referidos e, sempre que possível, avaliação oftalmológica (com exame da úvea anterior pela técnica de lâmpada de fenda), eletrocardiograma (se necessário, ecocardiografia), tomografia computadorizada do tórax, fibrobroncoscopia com biópsia transbrônquica e lavado broncoalveolar, e ecografia abdominal total.
Raramente, faz-se cintilografia com gálio-67. Não se realiza teste de Kveim, dosagem sérica de enzima conversora de angiotensina e pesquisas de interleucinas, interferon, TNF e outras em nível de biologia molecular. Como o Serviço de Cirurgia Torácica está bastante integrado com a Pneumologia Clínica, freqüentemente os pacientes são encaminhados diretamente para biópsia de gânglios mediastinais ou pulmonar a céu aberto e chegam ao pneumologista apenas após o procedimento.
O estudo radiológico convencional do tórax incluía incidências padrão em frontal e perfil com esôfago opacificado, e, também, um radiograma penetrado do mediastino.
A avaliação funcional pulmonar constou de espirometria, na maioria dos casos, com determinação da capacidade vital forçada, do volume expiratório forçado no primeiro segundo e da relação entre eles. A medida dos volumes pulmonares e da capacidade difusiva não foi realizada na maio-ria dos casos. A equação e tabela de normalidade usadas para a sua interpretação foram as de Knudson, de 1983.
Excluindo-se outras causas, as manifestações clínicas foram atribuídas à sarcoidose, e foram classificadas em: ausência de sintomas (paciente que não apresentou sinal ou sintoma algum, ou quando o achado não pudesse ser atribuível à sarcoidose); sintomas pulmonares (tosse, dispnéia, dor torácica); manifestações cutâneas (alteração cutânea provavelmente associada à sarcoidose, particularmente eritema nodoso); manifestações articulares (artralgias, edema articular); manifestações sistêmicas (febre, emagrecimento, sudorese noturna); outras manifestações (cardiológicas, oculares, ou de acometimento do sistema nervoso central).
Utilizou-se a classificação radiológica habitual, recomendada pelo consenso das sociedades American Thoracic Society, European Respiratory Society e World Association of Sarcoidosis and Other Granulomatous Disorders,(1) incluindo-se os tipos radiológicos 0, I, II, III e IV (0 - radiograma normal, I - adenopatias hilares bilaterais e mediastinais, II - adenopatias e infiltração pulmonar, III - apenas infiltração pulmonar, IV - fibrose pulmonar), sendo todos os casos reavaliados pelos radiologistas do serviço. Os autores preferem a expressão "tipo" a "estágio" devido à sarcoidose ser uma doença sistêmica em que os achados de imagem do tórax freqüentemente não refletem sua fase evolutiva ou gravidade global. A tomografia computadorizada de alta resolução costuma mostrar aspectos típicos da doença, mas por motivos econômicos não foi realizada de rotina.
Os espécimes para exame histopatológico foram obtidos por biópsia endobrônquica e/ou transbrônquica (através de fibrobroncoscopia), mediastinoscopia ou biópsia pulmonar a céu aberto. Em poucos casos, a comprovação histopatológica foi realizada a partir de biópsia de estrutura superficial (gânglio ou pele).
O quadro histopatológico compatível com sarcoidose incluía achados como: granuloma não caseoso, bem-formado, abundantes células epitelióides e gigantócitos multinucleados, circundados por um anel de linfócitos.
Os pacientes, na sua maioria, receberam inicialmente 40 mg de prednisona em dias alternados, com redução progressiva, a cada três meses, perfazendo um total de doze a 24 meses de tratamento. Nenhum recebeu medicamentos imunossupressores como metotrexato, azatioprina ou ciclofosfamida, antimaláricos (hidroxicloroquina) e nem bloqueadores do fator de necrose tumoral.
Os dados clínicos e laboratoriais foram analisados estatisticamente de forma univariada. O teste de Kolmogorov-Smirnov foi utilizado para avaliar a normalidade dos dados, sendo a significância dos testes baseada nas probabilidades de Liliefors. Variáveis contínuas com distribuição normal foram comparadas por meio do teste t de Student, sendo os valores expressos em média e desvio padrão. Variá-veis contínuas sem distribuição normal foram comparadas pelo teste de Wilcoxon-Mann-Whitney, tendo seus valores expressos por mediana, amplitude interquartílica, média e desvio-padrão. A comparação de médias em mais de dois grupos simultâneos foi realizada com a análise de variância. Variáveis alocadas em categorias foram comparadas usando-se o teste do qui-quadrado, incluindo o teste de Fisher. Alguns valores foram distribuídos em porcentagem do grupo. A significância foi definida como erro tipo I menor que 0,05. A análise foi processada utilizando-se o programa Statistical Package for Social Science versão 11.0.
RESULTADOSO grupo foi constituído por 92 pacientes, 53 do sexo feminino (58%) e 39 do masculino (42%), com média de idade de 41,8 ± 14,1 anos, variando entre 11 e 78 anos. Homens e mulheres não diferiram significativamente quanto à idade: respectivamente, 40,1 ± 14,4 versus 43,1 ± 13,9 anos (p = 0,32). Quanto à origem étnica, 77 eram caucasianos (84%), enquanto que 15 eram não caucasianos (16%). Quanto ao tabagismo, 8 pacientes eram fumantes (10%), 24 ex-fumantes (29%), e 51 nunca fumaram (61%) (Figura 1).

Quanto à relação entre sexo e idade, houve predomínio de mulheres, com 46 casos no grupo de pacientes com idade acima de 30 anos (87%), enquanto que entre os homens, 27 casos foram diagnosticados nesta faixa (69%), uma diferença significativamente menor (p = 0,04) (Figura 2).

No momento do diagnóstico de sarcoidose, apenas 11 indivíduos eram assintomáticos (12%). A freqüência de sintomas foi igual em homens e mulheres (87% e 89%, respectivamente; p = 0,83). Também não houve diferença entre homens e mulheres na apresentação de sintomas torácicos (79% versus 92%; p = 0,47), assim como na apresentação de sintomas extratorácicos (82% versus 77%; p = 0,53).
Entre os pacientes sintomáticos, 61 apresentavam sintomas torácicos (66%) e 64 apresentavam sintomas extratorácicos e sistêmicos (70%). Ocorreram sintomas exclusivamente torácicos em 17 casos (18%) e exclusivamente extratorácicos em 20 casos (22%); 44 apresentavam, concomitantemente, sintomas torácicos e extratorácicos, e também sistêmicos (48%). Dos sintomas torácicos, a tosse foi o mais freqüente, sendo referido por 45 pacientes (49%), seguindo-se dispnéia, por 38 (41%), e dor torácica por 17 (19%). Dentre as manifestações extratorácicas e sistêmicas, as mais freqüentes foram: emagrecimento em 24 casos (26%); febre em 19 (21%); astenia em 15 (16%); adenopatias periféricas em 14 (15%) e artralgias em 13 casos (14%). Alterações cutâneas ocorreram em 10 pacientes (11%), sendo que eritema nodoso foi diagnosticado em 6 (7%). Alterações oftalmológicas ocorreram em 6 pacientes (7%) e cardiológicas em 3 (3%). Episódios de litíase urinária ocorreram em 5 pacientes (5%) (Tabela 1).

No grupo de pacientes sintomáticos, o tempo médio transcorrido entre o início dos sintomas e a consulta médica foi de 6,1 ± 7 meses, sendo que 59% dos pacientes procuraram atendimento médico em até 3 meses.
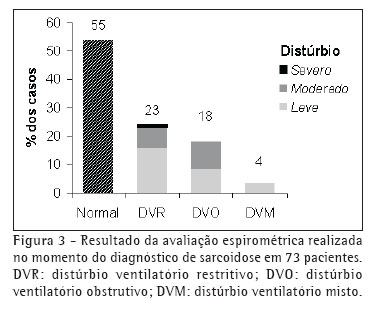
A avaliação espirométrica (espirometria simples) foi realizada, por ocasião do diagnóstico, em 73 pacientes (79%), tendo sido normal em 40 deles (55%).
Distúrbio ventilatório restritivo ocorreu em 17 pacientes (23%), distúrbio ventilatório obstrutivo em 13 (18%), e distúrbio ventilatório misto em 3 (4%). Nestes casos em que houve alteração espirométrica (33 casos), o distúrbio ventilatório foi de intensidade leve em 20 casos (28% de 73 pacientes avaliados) e de intensidade moderada em 13 (18% de 73 pacientes avaliados). Distúrbio ventilatório grave não foi registrado neste grupo (Figura 3).
Entre os pacientes que realizaram espirometria, foram encontradas alterações da função pulmonar em 58% dos homens (18 pacientes) e em 36% das mulheres (15 pacientes), sendo essa diferença sem significância estatística (p = 0,058).
A medida da calciúria de 24 horas foi realizada em 49 pacientes (53%), encontrando-se calciúria superior a 300 mg/24h em 12 casos (24% dos pacientes avalia-dos), e tendo como média 225,4 ± 145,8 mg/24h.
Quanto ao estudo radiológico de tórax, foi possível recuperar os radiogramas de 78 pacientes, todos estes referentes ao momento do diagnóstico. Dentre estes casos, 23 pacientes apresentavam tipo radiológico I (30%), 38 classificação radiológica tipo II (48%) e 17 tipo radiológico III (22%). Nenhum caso foi classificado como tipo IV (fibrose pulmonar) e nenhum paciente apresentou radiograma de tórax normal no momento do dia-gnóstico (Figura 4).

Os espécimes para exame anatomopatológico tiveram origem intratorácica em 84 pacientes (91%): por mediastinoscopia em 46 (50%), biópsia transbrônquica em 19 (21%) e biópsia a céu aberto em 19 deles (21%). Biópsia de linfonodo periférico foi realizada em 5 pacientes (6%), e tegumentar em 3 (3%).
Como medida terapêutica principal, a corticoterapia sistêmica foi indicada em 55 pacientes (60%), incluindo todos os do tipo radiológico III, sendo os demais do tipo II. Não foram observados efeitos adversos significativos que motivassem a suspensão da corticoterapia.
Algumas correlações entre diversas variáveis foram realizadas para se verificar a significância e a importância prática das mesmas.
Os pacientes que apresentaram episódios de febre como sintoma inicial de sarcoidose procuraram o médico em um tempo significativamente menor que aqueles que não a apresentaram no início do quadro (2,6 ± 2,5 versus 7,4 ± 7,7 meses; p = 0,009).
Pacientes do sexo masculino apresentaram níveis de calciúria urinária de 24h significativamente maiores que aqueles do sexo feminino (288,5 ± 171,0 versus 184,1 ± 111,5mg/dL; p = 0,014).
Quando se comparou o tipo radiológico com a média da calciúria urinária, encontrou-se que o grupo de pacientes com tipo radiológico III teve calciúria média significativamente maior que os pacientes com tipos radiológicos I ou II: tipo I com média de 198,6 ± 107,3; tipo II com média de 213,2 ± 112,2; e tipo III com média de 349,6 ± 181,3. A análise de variância mostrou haver diferença significativa entre o tipo III e os tipos I e II (p = 0,011).
Até o momento, no Pavilhão Pereira Filho, nenhum paciente com sarcoidose foi submetido a transplante pulmonar, sendo esta mais uma indicação de que a doença, em nosso meio, não compromete os pulmões com extrema gravidade, a ponto de levar à insuficiência respiratória.
DISCUSSÃO No presente estudo, avaliaram-se retrospectivamente pacientes com diagnóstico de sarcoidose atendidos em um hospital especializado em doenças respiratórias. Pelas características da amostra, não se pode afirmar que os resultados obtidos possam ser extrapolados para a população dos pacientes com sarcoidose, mas de qualquer maneira poderá representar um perfil a ser utilizado como referência para a prática médica em nosso meio.
A seguir, estabelecem-se algumas correlações entre os dados observados neste estudo e em séries da literatura.
Inicialmente, deve-se analisar alguns dados de um estudo anterior da casuística do Pavilhão Pereira Filho, que incluiu 138 casos de sarcoidose diagnosticados entre 1965 e 1989, com as seguintes características: idade - média de 30,7 anos, 21 casos abaixo de 20 anos (15%), 91 casos entre 20 e 40 anos (66%), e 26 casos acima de 40 anos (19%); sexo - feminino em 79 casos (57%) e masculino em 59 casos (43%); cor - branca em 106 casos (77%) e negra em 32 casos (23%).(29)
A presente série representa a seqüência temporal deste primeiro grande estudo sobre sarcoidose realizado no Pavilhão Pereira Filho. Quanto às características dos pacientes, verifica-se semelhança entre ambas, com exceção da faixa etária, pois nas duas últimas décadas os pacientes com sarcoidose apresentaram idade mais avançada. Enquanto a média atual é de 41,8 anos, anteriormente era de 30,7 anos. Este aumento da faixa etária também foi observado em outros estudos como o denominado A Case Control Etiologic Study of Sarcoidosis, nos EUA, onde a média de idade esteve acima de 40 anos(30), e outro, na Holanda, cuja média foi de 46,7 anos.(11) Em alguns países, como Suécia e Japão, observou-se um segundo pico de incidência na sexta década de vida, especialmente entre as mulheres.
O estudo A Case Control Etiologic Study of Sarcoidosis, projeto norte-americano multicêntrico, realizado por um grupo de pesquisadores de dez grandes centros clínicos, teve como um de seus objetivos determinar os locais (órgãos) envolvidos no grupo de pacientes como um todo e em subgrupos diferenciados por sexo, raça e idade.(30-31) Esta população era heterogênea quanto à raça (53% brancos, 44% negros), sexo (64% mulheres, 36% homens), e idade (46% abaixo de 40 anos, 54% com 40 anos ou mais). As mulheres tinham mais envolvimento ocular, neurológico, eritema nodoso, e idade acima de 40 anos, enquanto que os homens tinham mais hipercalcemia. Os negros tinham mais envolvimento cutâneo (excetuado o eritema nodoso), ocular, hepático, de medula óssea e de linfonodos extratorácicos. Os autores concluíram que a apresentação inicial da sarcoidose tem relação com sexo, idade e, muito particularmente, com a raça negra.
Nos EUA, a sarcoidose é mais freqüente em afro-americanos do que em caucasianos, com uma incidência anual ajustada de 35,5 e de 10,9 por 100.000 habitantes, respectivamente.(1) Em termos mundiais, entretanto, aproximadamente 80% dos pacientes são brancos. No nosso estudo, observa-se também esta tendência, embora de menor proporção, uma vez que 16% dos casos são de indivíduos de cor negra. Lembre-se que no Rio Grande do Sul, segundo o Instituto Brasileiro de Geografia e Estatística, 4% da população é de cor negra.(32) A raça predominante nesta amostra foi caucasiana (84%), o que discorda de outros levantamentos da literatura. Um potencial viés socio-econômico pode ser observado na amostra, visto que grande parte dos pacientes era provinda de assistência de saúde privada. Achados semelhantes foram observados em estudos de populações com as mesmas características.(5)
O pequeno predomínio de mulheres na amostra (58%), em relação aos homens (42%), é semelhante ao que se observa nas séries em geral.(11,33) Em um estudo populacional, a incidência de sarcoidose entre pacientes captados através de uma organização de saúde foi de 21,6 mulheres e 15,3 homens por 100.000 habitantes/ano.(34) A idade média na ocasião do diagnóstico foi de 40,9 anos, em ambos os grupos. Esses dados coincidem com outros estudos em relação às mulheres.(5) No estudo A Case Control Etiologic Study of Sarcoidosis, abaixo dos 40 anos há um predomínio de diagnóstico em homens.(30)
O tabagismo foi um achado infreqüente (10%), o que pode contribuir para o diagnóstico precoce, pois diminui o fator de confusão dos sintomas respiratórios associados. Embora alguns autores tenham concluído que fumar protege contra a sarcoidose, ainda não se obteve evidência que suporte esta afirmação.(35)
A sarcoidose freqüentemente apresenta-se sem manifestações clínicas ou com sintomas de pequena intensidade, o que, por um lado, pode retardar seu diagnóstico e, por outro, pode auxiliar sobremaneira no diagnóstico diferencial. Esta é uma característica encontrada na maioria das séries da literatura. Em outros estudos também se constata um retardo no diagnóstico da sarcoidose, o que parece ocorrer mais pelas características da apresentação da doença do que por características do paciente ou do médico.(36)
O órgão isoladamente mais afetado foi o pulmão, o que se expressa pelo achado de 75% de sintomáticos torácicos, valor coincidente com os de outros estudos, que apresentam incidência variável entre 50% e 95%. Sintomas pulmonares isolados podem explicar retardo no diagnóstico, principalmente pela ausência de especificidade dos mesmos.(6) Esta variável não foi avaliada no presente estudo. O tempo médio entre o surgimento de sintomas e a primeira consulta foi de seis meses, sendo a grande maioria dos pacientes diagnosticada com até três meses de presença de sintomas (59%). Dos sintomas extratorácicos, os mais comuns foram emagrecimento, febre e astenia, que caracterizam o componente sistêmico da doença. Fadiga persistente foi referida em uma série como o principal sintoma de apresentação da sarcoidose (71% dos casos).(11) Na presente série, ocorreu em 16% dos pacientes. Naquela série foi realizado um estudo através de questionário dirigido aos membros da Sociedade Holandesa de Sarcoidose, sendo que foram obtidas 1.026 respostas (58% do total de questionários enviados). A idade média foi de 46,7 + 11,6 anos e 63% dos pacientes eram mulheres. Havia 176 casos de sarcoidose familiar. Os sintomas mais freqüentes foram: fadiga (71%), dispnéia (70%), artralgias (52%), mialgias (39%) e dor torácica (27%). Foi usada corticoterapia sistêmica em 565 pacientes (55,1%).
Embora a apresentação radiológica da presente série não seja significativamente diferente das relatadas na literatura, deve-se referir que enquanto nela 30% dos casos eram do tipo radiológico I, outros autores referem este tipo em 40% a 50% dos seus pacientes; já o tipo II, apresentado por 48% dos casos desta série, costuma ocorrer em menos de 30% nas séries da literatura; e o tipo III observado em 22% aproxima-se do valor encontrado na literatura.(3-4,29,33) O fato de não termos casos do tipo 0 (radiograma normal) pode ser explicado, em parte, por nosso serviço ser especia-lizado em pneumologia, o que dificulta o ingresso de pacientes sem anormalidades radiológicas do tórax. Em nosso serviço, não costumamos classificar pacientes no tipo IV, por ocasião do diagnóstico, devido à impossibilidade de assegurar, nesse momento, a existência exclusiva de componente fibrótico, que é o que caracteriza este grupo. Só se pode afirmar que um caso é do tipo IV quando existem anormalidades sugestivas de fibrose e com estabilidade lesional por um período longo de acompanhamento, e sem outras lesões passíveis de reversibilidade.
Os resultados da espirometria indicam que a sarcoidose geralmente não tem grande impacto funcional pulmonar, uma vez que mais da metade dos pacientes teve o exame normal, e quando alterado, geralmente a disfunção foi de pequena intensidade. O padrão do distúrbio ventilatório pode ser tanto obstrutivo quanto restritivo, dependendo da distribuição das lesões (parênquima pulmonar versus vias aéreas) e da presença de co-morbidades.
A escolha dos procedimentos diagnósticos utilizados nos pacientes desta série dependeu da experiência dos profissionais do serviço e da disponibilidade de equipamentos. A experiência com mediastinoscopia dos cirurgiões e as freqüentes dificuldades do setor de endoscopia, por vezes, interferiram na escolha da técnica para biópsia. Muitos pacientes já chegaram ao serviço com biópsia feita ou foram encaminhados diretamente ao cirurgião. E uns poucos, inicialmente, tinham como maior suspeita, pneumonia intersticial fibrosante, daí terem sido submetidos a biópsia por toracotomia. Atualmente, a técnica preferencial para obtenção de material para exame anatomopatológico, em pacientes com suspeita de sarcoidose, sem dúvida, é a fibrobroncoscopia, pois possibilita colher, num mesmo tempo, fragmentos de tecido para exame anatomopatológico e material de lavado para análise de diversos itens.
Para pacientes do tipo radiológico I, em que o diagnóstico de sarcoidose é de longe o mais provável, e sem indicação de corticoterapia, mais freqüentemente não temos realizado biópsia, uma vez que estes pacientes devem ficar apenas em observação.
A corticoterapia foi indicada segundo os critérios recomendados pela literatura, ultimamente uniformizados pelos consensos internacionais, sendo utilizada por cerca de metade dos pacientes da série, o que se assemelha aos outros estudos. Nossa preferência pelo seu uso em dias alternados, da mesma forma que o uso diário, não tem respaldo satisfatório na literatura, mas tem-se mostrado eficaz em nosso serviço.
Diversas outras correlações de achados desta série, citadas nos resultados, como, por exemplo, entre idade, sexo, cor, sintomas, tipos radiológicos, calciúria e sintomas extratorácicos deverão ser, futuramente, melhor avaliadas, uma vez que o estudo foi retrospectivo e o número de casos limitado.
As características dos pacientes com sarcoidose desta série, provenientes na sua maioria do Estado do Rio Grande do Sul, não diferem significativamente das encontradas na literatura, quando analisadas no seu conjunto.(37) O fato de não havermos detectado nenhum caso que tivesse recebido tratamento antituberculoso, anteriormente ao diagnóstico de sarcoidose, pode ser explicado, pelo menos em parte, pelos padrões de exigência do Programa de Controle da Tuberculose do Estado do Rio Grande do Sul e pela grande acurácia dos laudos radiológicos do nosso serviço (e também de outros) para a suspeita de sarcoidose.
A possibilidade de muitos pacientes não serem diagnosticados, a falta de notificação dos casos reconhecidos, o desconhecimento da causa, as dificuldades diagnósticas (o diagnóstico é de exclusão), e a impossibilidade de intervenção terapêutica específica tornam a sarcoidose uma doença com muitas incógnitas e de difícil entendimento etiopatogênico. No entanto, ela apresenta alguns padrões clínicos que possibilitam seu reconhecimento e, como regra, a conduta pode ser tomada com base nas recomendações dos consensos, e, desta forma, o pneumologista ou outro especialista dedicado ao setor, na maioria dos casos, pode utilizar critérios acessíveis para diagnosticar e tratar seus pacientes.(1-2)
Como estudos epidemiológicos comparativos demonstraram que fatores geográficos, étnicos e genéticos têm associação com características específicas dos pacientes com sarcoidose, recomenda-se a realização de mais estudos de séries de casos em diferentes regiões.
REFERÊNCIAS 1. American Thoracic Society (ATS), European Respiratory Society (ERS) and World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG): Statement on sarcoidosis. Joint Statement of the American Thoracic Society, ERS and WASOG. Am J Respir Crit Care Med. 1999;160(2):736-55.
2. Costabel U, Hunninghake GW. ATS/ERS/WASOG statement on sarcoidosis. Sarcoidosis Statement Committee. American Thoracic Society. European Respiratory Society. World Association for Sarcoidosis and Other Granulomatous Disorders . Eur Respir J. 1999;14(4):735-7.
3. Crofton J, Douglas AC. Sarcoidosis. In: Crofton J, Doublas AC. Respiratory diseases. 3rd ed. Oxford: Blackwell; 1981.
4. James DG. Clinical concepts of sarcoidosis. Am Rev Respir Dis. 1961;84(Pt 2):66-70.
5. Judson MA, Baughman RP, Teirstein AS, Terrin ML, Yeager H Jr. Defining organ involvement in sarcoidosis: the ACCESS proposed instrument. Sarcoidosis Vasc Diffuse Lung Dis. 1999;16(1):75-86.
6. Johns, CJ, Michele, TM. The clinical management of sarcoidosis: a 50-year experience at the Johns Hopkins Hospital. Medicine. 1999;78:65-111.
7. DeRemee RA. Sarcoidosis. Mayo Clin Proc. 1995;70(2): 177-81.
8. Tarantino AB, Corrêa da Silva LC. Sarcoidose. In: Tarantino AB. Doenças pulmonares. 5a ed. Rio de Janeiro: Guanabara Koogan; 2002. p.814-26.
9. Reich JM. What is Sarcoidosis? Chest. 2003;124(1):367-71.
10. Wurm K, Rosner R. Prognosis of chronic sarcoidosis. Ann NY Acad Sci. 1976;278:732-5.
11. Wirnsberger RM, de Vries J, Wouters EF, Drent M. Clinical presentation of sarcoidosis in the Netherlands an epidemiological study. Neth J Med. 1998;53(2):53-60.
12. Hills SE, Parkes SA, Baker SB. Epidemiology of sarcoidosis in the Isle of man-2: evidence for space-time clustering. Thorax. 1987;42(6):427-30.
13. Hiraga Y. An epidemiological study of clustering of sarcoidosis cases. Nippon Rinsho. 1994;52(6):1438-42. Japanese.
14. Panayeas S, Theodorakopoulos P, Bouras, Constantopoulos S. Seasonal occurrence of sarcoidosis in Greece. Lancet. 1991;338(8765):510-1.
15. Bardinas F, Morera J, Fite E, Plasencia A. Seasonal clustering of sarcoidosis. Lancet. 1989;2(8660):455-6.
16. Hosoda Y, Yamaguchi M, Hiraga Y. Global epidemiology of sarcoidosis. What story do prevalence and incidence tell us? Clin Chest Med. 1997;18(4):681-94.
17. Loddenkemper R, Kloppenborg A, Schoenfeld N, Grosser H, Costabel U. Clinical findings in 715 patients with newly detected pulmonary sarcoidosis - Results of a cooperative study in former West Germany and Switzerland. Sarcoidosis Vasc Diffuse Lung Dis. 1998;15(2):178-82.
18. Fite E, Alsina JM, Mana J, Pujol R, Ruiz J, Morera J. Epidemiology of sarcoidosis in Catalonia: 1979-1989. Sarcoidosis Vasc Diffuse Lung Dis. 1996;13(2):153-8.
19. Pietinalho A, Ohmichi M, Hiraga Y, Lofroos AB, Selroos O. The mode of presentation of sarcoidosis in Finland and Hokkaido, Japan. A comparative analysis of 571 Finnish and 686 Japanese patients. Sarcoidosis Vasc Diffuse Lung Dis. 1996;13(2):159-66.
20. Corrêa da Silva LC. Sarcoidose. In: Corrêa da Silva LC. Condutas em pneumologia. Rio de Janeiro: Revinter; 2001. p.494-505.
21. Winterbauer RH, Belie N, Moores KN. A clinical interpretation of bilateral hilar adenopathy. Ann Intern Med. 1973;78:65-71.
22. Bethlem N, Bethlem EP, Lemle A, Capone D, Souza GRM, Corrêa JC et al. Revisão e sugestões de normas para o diagnóstico, tratamento e acompanhamento da sarcoidose gangliopulmonar. J Pneumol. 1995;21(3):123-31.
23. Mitchell DN, Scadding JG, Heard BE, Hinson KF. Sarcoidosis: histopathological definition and clinical diagnosis. J Clin Pathol. 1977;30(5):395-8.
24. Baughman RP, Ianuzzi MC. Editorial - Diagnosis of sarcoidosis: When is a peek good enough? Chest 2000; 117:(4)931-2.
25. Judson MA. An approach to the treatment of pulmonary sarcoidosis with corticosteroids: the six phases of treatment. Chest. 1999;115(4):1158-65.
26. Paramothayan S, Jones PW. Corticosteroid therapy in pulmonary sarcoidosis. A systematic review. JAMA. 2002;287(10):1301-7.
27. Neville E, Walker NA, James DG. Prognostic factors predicting the outcome of sarcoidosis: an analysis of 818 patients. Q J Med. 1983;52(208):525-33.
28. James DG. Life-threatening situations in sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 1998;15(2):134-9.
29. Pereira, M. Sarcoidose: análise de 138 casos [tese]. Porto Alegre:Universidade Federal do Rio Grande do Sul; 1994. 128 p.
30. Baughman RP, Teirstein AS, Judson MA, Rossman MD, Yeager H, Bresnitz EA; Control Etiologic Study of Sarcoidosis (ACCESS) research group, et al. Clinical characteristics of patients in a case control study of sarcoidosis. Am J Respir Crit Care Med. 2001;164(10 Pt 1):1885-9.
31. Design of a case control etiologic study of sarcoidosis (ACCESS). ACCESS Research Group. J Clin Epidemiol. 1999;52(12):1173-86.
32. IBGE. Instituto Brasileiro de Geografia e Estatística. Recenseamento geral do Brasil: Censo demográfico 2000. Rio de Janeiro; 2001.
33. James DG, Neville E, Siltzbach LE. A worldwide review of sarcoidosis. Ann N Y Acad Sci. 1976;278:321-34.
34. Rybicki BA, Major M, Popovich J Jr, Maliarik MJ, Iannuzzi MC. Racial differences in sarcoidosis incidence: a 5-year study in health maintenance organization. Am J Epidemiol. 1997;145(3):234-41.
35. Peros-Golubicic T, Ljubic S. Cigarette smoking and sarcoidosis. Acta Med Croatica. 1995;49(4-5):187-93.
36. Judson MA, Thompson BW, Rabin DL, Steimel J, Knattereud GL, Lackland DT; ACCESS Research Group, et al. The diagnostic pathway to sarcoidosis. Chest. 2003;123(2):406-12.
37. Corrêa da Silva LC, Hertz FT, Caraver F, Cruz DB, Fernandez JC, Fortuna FP et al. Demographical, clinical, lung functional and radiological findings of patients with sarcoidosis in South of Brazil. Am J Respir Crit Care Med. 2004; 169(7):A36.
_________________________________________________________
* Trabalho realizado no Pavilhão Pereira Filho (PPF) - Serviço de Pneumologia, Cirurgia Torácica e Radiodiagnóstico do Complexo Hospitalar da Santa Casa de Porto Alegre. Disciplina de Pneumologia da Fundação Faculdade Federal de Ciências Médicas de Porto Alegre (FFFCMPA). Programa de Pós-Graduação (PPG) em Medicina: Pneumologia da Universidade Federal do Rio Grande do Sul - UFRGS - Porto Alegre (RS) Brasil. Trabalho financiado parcialmente pela FAPERGS - Fundação de Assistência à Pesquisa do Rio Grande do Sul
1. Professor Responsável pela Disciplina de Pneumologia da Fundação Faculdade Federal de Ciências Médicas de Porto Alegre - FFFCMPA - Porto Alegre (RS) Brasil.
2. Acadêmicos de Medicina da Fundação Faculdade Federal de Ciências Médicas de Porto Alegre -FFFCMPA - Porto Alegre (RS) Brasil.
3. Mestrando no Pavilhão Pereira Filho - PPG em Medicina: Pneumologia, Universidade Federal do Rio Grande do Sul - UFRGS - Porto Alegre (RS) Brasil.
4. Pneumologista. Ex-Residente do Pavilhão Pereira Filho - PPF - Porto Alegre (RS) Brasil.
5. Radiologista do Pavilhão Pereira Filho - PPF - Porto Alegre (RS) Brasil.
6. Diretor do Setor de Radiodiagnóstico do Pavilhão Pereira Filho - PPF - Porto Alegre (RS) Brasil.
Endereço para correspondência: Luiz Carlos Corrêa da Silva. Rua Pedro Ivo 532/302, CEP: 90450-210, Bela Vista, Porto Alegre (RS) Brasil. Tel/Fax: 55 51 3221.8522. E-mail: lccsilva@yahoo.com.br
Recebido para publicação em 21/7/04. Aprovado, após revisão, em 2/5/05.











 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket