ABSTRACT
Exposure to radon can impact human health. This is a nonsystematic review of articles written in English, Spanish, French, or Portuguese published in the last decade (2013-2023), using databases such as PubMed, Google Scholar, EMBASE, and SciELO. Search terms selected were radon, human health, respiratory diseases, children, and adults. After analyzing the titles and abstracts, the researchers initially identified 47 studies, which were subsequently reduced to 40 after excluding reviews, dissertations, theses, and case-control studies. The studies have shown that enclosed environments such as residences and workplaces have higher levels of radon than those outdoors. Moreover, radon is one of the leading causes of lung cancer, especially in nonsmokers. An association between exposure to radon and development of other lung diseases, such as asthma and COPD, was also observed. It is crucial to increase public awareness and implement governmental control measures to reduce radon exposure. It is essential to quantify radon levels in all types of buildings and train professionals to conduct such measurements according to proven efficacy standards. Health care professionals should also be informed about this threat and receive adequate training to deal with the effects of radon on human health.
Keywords:
Radon; Lung neoplasms; Risk factors.
RESUMO
A exposição ao radônio pode ter impacto na saúde humana. Esta é uma revisão não sistemática de artigos escritos em inglês, espanhol, francês ou português publicados na última década (2013-2023), utilizando bancos de dados como PubMed, Google Acadêmico, EMBASE e SciELO. Os termos de busca selecionados foram radônio, saúde humana, doenças respiratórias, crianças e adultos. Após a análise dos títulos e resumos, os pesquisadores inicialmente identificaram 47 estudos, que foram posteriormente reduzidos para 40 após a exclusão de revisões, dissertações, teses e estudos de caso-controle. Os estudos mostraram que ambientes fechados como residências e locais de trabalho apresentam maiores níveis de radônio do que ambientes externos. Além disso, o radônio é uma das principais causas de câncer de pulmão, especialmente em não fumates. Também foi observada associação entre exposição ao radônio e desenvolvimento de outras doenças pulmonares, como asma e DPOC. É crucial aumentar a conscientização do público e implementar medidas governamentais de controle para reduzir a exposição ao radônio. É fundamental quantificar os níveis de radônio em todos os tipos de edifícios e treinar profissionais para realizar essas medições segundo padrões de eficácia comprovada. Os profissionais de saúde também devem ser informados sobre essa ameaça e receber formação adequada para lidar com os efeitos do radônio na saúde humana.
Palavras-chave:
Radônio; Neoplasias pulmonares; Fatores de risco.
INTRODUÇÃO O radônio é um gás radioativo incolor e inodoro que possui meia-vida de 3,83 dias. É formado a partir da decomposição radioativa do urânio das águas subterrâneas, do solo ou das rochas, e seus produtos também são incolores, insípidos e inodoros.(1,2)
As concentrações de radônio em ambientes internos (casas e edifícios) variam e são influenciadas por várias condições: (a) características geológicas do local (permeabilidade das rochas, teor de urânio e tipo de solo onde o edifício está localizado); (b) caminhos que o radônio encontra para se infiltrar em residências e em edifícios comerciais ou não comerciais; (c) emanação de radônio de materiais de construção e ornamentação (como pisos e paredes de granito); (d) taxa de troca de ar entre áreas internas e externas, que depende do tipo de edifício, dos sistemas de ventilação e da estanqueidade (vedação) do edifício.(3)
Os sintomas inespecíficos experimentados pelos ocupantes em virtude do tempo passado em um edifício com má qualidade do ar interno são coletivamente chamados de “síndrome do edifício doente”.(4) O radônio é prejudicial à saúde dos indivíduos expostos a ele. Conhecer os riscos dessa exposição é fundamental para evitar danos à saúde.(5)
O radônio penetra nos edifícios através de rachaduras em pisos ou juntas de paredes, espaços ao redor de canos e fios, pequenos poros em paredes feitas de blocos ocos de concreto e paredes ou tetos abertos. Geralmente atinge concentrações mais altas em porões e em cômodos em contato direto com o solo, mas concentrações significativas também podem ser encontradas acima do piso térreo. (3) Essas concentrações podem variar entre edifícios adjacentes e dentro da mesma estrutura de um dia para o outro, ou mesmo dentro de horas.(3)
A unidade de medida do radônio é o Becquerel por metro cúbico (Bq/m3),(6) e a concentração média de radônio ao ar livre varia de 5 Bq/m3 a 15 Bq/m3; entretanto, é maior em espaços fechados, especialmente se forem mal ventilados. Em edifícios como escolas, escritórios e residências, as concentrações de radônio variam de 10 Bq/m3 a mais de 10.000 Bq/m3.(7,8)
A OMS recomenda que as concentrações de radônio em ambientes internos não ultrapassem 100 Bq/m3.(4) É aconselhável que o nível de referência não ultrapasse 300 Bq/m3.(7,8) Segundo a Comissão Internacional de Proteção Radiológica,(9) a dose efetiva global atribuída a esse tipo de radiação é estimada em 2,4 mSv/ano. A soma das doses equivalentes nos tecidos ou órgãos é a dose efetiva.
O Projeto Planalto de Poços de Caldas,(10) uma iniciativa pioneira no Brasil, tem como objetivo fornecer informações confiáveis, tecnicamente precisas e eticamente seguras para alertar os profissionais de saúde e a população sobre os efeitos da radiação do radônio na saúde. O estudo identificou três locais com doses médias acima de 10 mSv/ano, a saber: o Morro do Ferro (na zona rural da cidade de Poços de Caldas), o Morro do Taquari e uma mina de urânio (ambos na zona rural de cidade de Caldas).(10)
A segunda parte desse projeto (2004-2013) identificou que 21% dos domicílios pesquisados apresentavam concentração de radônio superior a 200 Bq/m3, apontando para a necessidade de implementação de um modelo permanente de vigilância da exposição à radiação natural.(11)
Em muitos países, a água potável é obtida de fontes subterrâneas, como nascentes e poços. Frequentemente, essas fontes apresentam maiores concentrações de radônio do que as águas superficiais de reservatórios, rios ou lagos. O radônio dissolvido na água potável é liberado no ar de ambientes internos; assim, a quantidade inalada através da respiração é mais significativa do que a ingerida por meio da água potável.(3)
Esses dados são confirmados por um estudo realizado em Porto Alegre (RS) que determinou as concentrações de radônio em amostras de água obtidas de aquíferos (fraturados pré-cambrianos e porosos cenozóicos) que alimentam essa cidade; constatou-se que mais da metade das amostras analisadas atingiram até 500 BqL,(12) valor acima do limite máximo determinado como seguro pela OMS.(3)
Segundo as propriedades do radônio, todos os edifícios são fontes potenciais desse gás, e sua concentração é única para cada ambiente. As pessoas que vivem ou trabalham nesses edifícios podem estar expostas a níveis muito altos, o que torna o problema mais complexo e de difícil abordagem.(6)
IMPACTOS DA EXPOSIÇÃO AO RADÔNIO NA SAÚDE HUMANA A exposição ao radônio dentro da residência pode causar sérios problemas de saúde. López et al. mostraram que as concentrações de radônio podem ser maiores em edifícios residenciais do que em edifícios públicos.(13)
É possível que a renovação do ar interno em edifícios residenciais ocorra apenas por um curto período, pois pode ocorrer ventilação inadequada à noite, durante o inverno ou durante o dia quando as pessoas estão fora. Isso foi confirmado durante a determinação das concentrações de radônio em residências canadenses: até três vezes maiores do que em edifícios escolares, 4,7 vezes maiores do que em outros edifícios públicos e locais de trabalho internos e 12 vezes maiores do que no ar de ambientes externos.(14)
Crianças em idade escolar expostas a medianas iguais ou superiores às concentrações recomendadas de material particulado fino, benzeno, limoneno, ozônio e radônio em ambiente escolar apresentaram significativamente mais sintomas sistêmicos, oculares e de vias aéreas superiores/inferiores (síndrome da escola doente) em comparação com indivíduos não expostos.(4,15)
Em escolas infantis, as concentrações de radônio em ambientes internos também são influenciadas pelos tipos de ventilação, pelo regime de frequência e pelas características do edifício.(16) Davis et al. constataram que as concentrações de radônio nas salas de aula diminuíram quando os sistemas de ventilação das escolas estavam ligados.(17) Branco et al. relataram que as concentrações de radônio em creches e escolas primárias de Portugal estavam relacionadas com o ano de construção dos edifícios.(18)
Vários fatores foram identificados como capazes de interferir nas concentrações de radônio em ambientes internos: número de ocupantes, ventilação, localização dos ambientes no edifício(19) e fatores relacionados à construção, pois construções localizadas no mesmo substrato geológico, mas com diferentes tipos de materiais de construção podem apresentar diferentes concentrações internas de radônio.(20,21) Além disso, a duração da exposição ao radônio também tem fundamental relevância. As crianças, por terem maior expectativa de vida, se expostas continuamente, apresentam maior risco de desenvolver câncer ao longo da vida.(22,23)
Outro tema destacado recentemente é o viés de ocupação no ambiente residencial. Casas recém-construídas são habitadas principalmente por pessoas mais jovens, que parecem estar expostas a maiores taxas de radiação (5,01 mSv/ano). Por outro lado, casas construídas há muitos anos são ocupadas por pessoas mais velhas que estão expostas a menores taxas de radiação (3,45-4,22 mSv/ano).(24) Essa observação é importante e reforça a citação anterior de que a exposição ao radônio quando se é mais jovem pode representar maior risco de problemas de saúde ao longo da vida.(22,23)
Um estudo realizado na região metropolitana do Recife (PE) constatou que as concentrações de radônio variaram de 2 a 1.174 Bq/m3 em residências de áreas com afloramentos de fosforito uranífero, aumentando em 10-16% o risco de desenvolvimento de neoplasia pulmonar relacionada ao radônio.(25) Os autores constataram que a maioria dos domicílios avaliados tinha hábitos que contribuíam para o acúmulo de gases em ambientes internos, como manter as janelas fechadas por muitas horas durante o dia.(25)
Altos níveis de radônio também foram documentados em grandes cidades, levando à maior exposição para uma população mais ampla.(8) Uma pesquisa realizada por Petroni & Lima(26) em 35 edifícios comerciais e residenciais com ar condicionado na cidade de São Paulo (SP) indicou que 3% deles apresentavam concentrações de radônio acima das recomendações da OMS.(3) O estudo em questão constatou a presença de radônio (acima de 4 mSv/ano) em alguns edifícios.
A população deve estar ciente dos impactos da exposição residencial ao radônio na saúde. Os profissionais de saúde devem incentivar o acesso a informações sobre os riscos à saúde decorrentes dessa exposição e informar sobre o monitoramento dos níveis residenciais de radônio fornecido pelos órgãos públicos.(27)
CÂNCER DE PULMÃO E RADÔNIO O câncer de pulmão é a principal causa de morte por câncer no mundo, além de ser um problema de saúde pública. O tabagismo é identificado como o principal fator de risco para o câncer de pulmão e é responsável por cerca de 80% dos casos, enquanto o radônio é o principal fator entre os indivíduos não fumantes, afetando entre 10% e 15% dessa população, e aumenta 25 vezes o risco entre os fumantes ativos em comparação com os não fumantes.(8,28,29)
Estudos sobre o câncer classificaram o radônio como um carcinógeno humano de grau I, também chamado de baixo grau ou bem diferenciado, por fazer com que as células cancerígenas sejam um pouco diferentes das células normais, o que faz com que a neoplasia progrida lentamente. Foi estabelecida uma relação entre a exposição ao radônio e o aumento do risco de câncer de pulmão na população geral.(8,30) No entanto, as consequências dessa contribuição variam entre os diferentes estudos.(31,32)
Os produtos de decaimento do radônio inalados emitem radiação associada a altos efeitos citotóxicos e genotóxicos, causando lesões no epitélio respiratório, danificando o DNA e potencialmente causando câncer de pulmão.(33)
Mecanismos de ação A carcinogênese por radiação é um processo complicado e sujeito aos efeitos de diferentes agentes ambientais, bem como a fatores genéticos. (34) O efeito carcinogênico induzido pela inalação de radônio, particularmente para o epitélio brônquico e especialmente nas bifurcações das vias aéreas, deve-se principalmente às progênies do radônio, principalmente o polônio 214 e o polônio 218, que emitem partículas alfa de alta energia como forma predominante de radiação. Apesar de sua capacidade limitada de penetrar nos tecidos, as partículas alfa podem danificar os tecidos expostos por apresentar alta eficácia biológica através de diversos efeitos citogenéticos.(34)
Alguns desses efeitos incluem a expressão de variantes patogênicas, aberrações cromossômicas, a geração de espécies reativas de oxigênio, a alteração dos ciclos celulares e o aumento da produção de proteínas associadas à regulação do ciclo celular e à carcinogênese.(35) Além disso, há evidências que sugerem que a exposição residencial ao radônio é capaz de induzir a expressão de variantes patogênicas de EGFR, translocações de ALK(31) e o aumento do risco de câncer de pulmão de pequenas células entre todos os tipos histológicos.(36,37)
O câncer de pulmão de células não pequenas apresenta alterações moleculares, como mutações somáticas (EGFR, BRAF, HER2, MET) ou rearranjos cromossômicos (ALK, ROS1, RET, NTRK) principalmente em não fumantes, sugerindo uma associação entre exposição ao radônio e câncer de pulmão de células não pequenas em não fumantes.(29)
Epidemiologia Estudos epidemiológicos estabeleceram uma importante associação entre exposição ao radônio e câncer pulmonar,(33,38-40) confirmada pela maior frequência de câncer pulmonar entre mineradores de urânio expostos ao radônio.(41,42)
Uma recente meta-análise de 13 estudos documentou uma relação direta entre o nível de radônio nos domicílios e o risco de desenvolver câncer de pulmão. Com base nessa informação, os autores estimaram que a exposição ao radônio possa ser responsável por até 2% das mortes por câncer de pulmão na Europa.(43)
O risco de câncer pulmonar aumenta com o nível de exposição ao radônio. Foi documentada uma associação entre exposição ao radônio acima de 50 Bq/m3 e câncer de pulmão.(44) Indivíduos expostos a concentrações superiores a 200 Bq/m3 tiveram um risco 2,06 vezes maior (IC95%: 1,61-2,64) do que aqueles expostos a concentrações ≤ 50 Bq/m3. Entre os fumantes ativos, o risco aumentou mais acentuadamente com o aumento da exposição ao radônio, chegando a ser até 29,3 vezes maior (IC95%: 15,4-55,7) para fumantes pesados expostos a concentrações superiores a 200 Bq/m3.(44)
Uma meta-análise avaliou a exposição ao radônio em ambientes internos e seus efeitos na saúde e mostrou um aumento no risco relativo de câncer pulmonar na China de 1,01 (IC95%:1,01-1,02) para cada incremento de 10 Bq/m3 nas concentrações internas de radônio.(45)
Uma revisão sistemática seguida de meta-análise(34) avaliou a associação entre exposição residencial ao radônio e risco de câncer pulmonar ao longo da vida em indivíduos que nunca fumaram. Aqueles expostos a concentrações de radônio ≥ 100 Bq/m3 apresentaram um excesso de risco relativo de 15% de desenvolver câncer de pulmão, especialmente os homens.
Outra meta-análise estudou a relação entre exposição residencial ao radônio e tipos histológicos de câncer pulmonar.(46) Alta exposição residencial ao radônio foi associada ao aumento do risco de câncer pulmonar (OR = 1,48; IC95%: 1,26-1,73). Todos os tipos histológicos de câncer pulmonar foram associados à exposição residencial ao radônio. A associação mais forte foi observada com o câncer de pulmão de pequenas células (OR = 2,03; IC95%: 1,52-2,71), seguido por adenocarcinoma (OR = 1,58; IC95%: 1,31-1,91), outros tipos histológicos (OR = 1,54; IC95%: 1,11-2,15) e carcinoma de células escamosas (OR = 1,43; IC95%: 1,18-1,74). Com a elevação dos níveis residenciais de radônio acima de 100 Bq/m3, o risco de câncer pulmonar, carcinoma pulmonar de pequenas células e adenocarcinoma aumentou em 11%, 19% e 13%, respectivamente.(46)
Exposição residencial A exposição residencial ao radônio é um importante contribuinte para a mortalidade por câncer pulmonar, embora essa contribuição seja altamente variável entre os diferentes países, indicando a necessidade de políticas específicas de prevenção. A correção das estimativas da altura das habitações é fundamental para fornecer estimativas confiáveis da mortalidade atribuível ao radônio.(31)
No Canadá, não existem áreas “livres de radônio”, e o radônio é responsável por 16% das mortes por câncer de pulmão; 20% das residências excedem a diretriz de 200 Bq/m3, e 47,5% excedem o nível de referência recomendado pela OMS (100 Bq/m3).(47-49)
A inalação prolongada de partículas alfa aumenta o risco de câncer pulmonar em 16% para cada incremento de 100 Bq/m3 e apresenta efeito sinérgico com outros fatores de risco para câncer pulmonar.(47) Quando os níveis atingem o limite estabelecido pela diretriz canadense, ou seja, acima de 200 Bq/m3, o risco de câncer pulmonar ao longo da vida é de 17% para os fumantes ativos e de 2% para os não fumantes.(47,50) Esses dados reforçam os observados por um estudo norte-americano no qual se observou um aumento de 3% na incidência de câncer pulmonar para cada aumento de 100 Bq/m3 na exposição ao radônio.(51)
Kurkela et al.(52) estimaram que (pelo menos) 3% a (no máximo) 8% de todos os cânceres pulmonares eram atribuíveis à exposição residencial ao radônio. A proporção de casos de carcinoma de pequenas células atribuíveis ao radônio foi de 8-13%. Entre os fumantes, a maioria dos casos relacionados ao radônio eram atribuíveis ao efeito combinado do radônio e do tabagismo, e os autores concluíram que a redução da exposição ao radônio para um nível de ação de 100 Bq/m3 eliminaria aproximadamente 30% dos casos de câncer de pulmão atribuíveis ao radônio.(52)
Hadkhale et al.,(53) em um estudo de base populacional na Finlândia, observaram um aumento do risco de câncer pulmonar em distritos hospitalares com alta exposição ao radônio em comparação com aqueles com menor exposição. Os autores relataram que a exposição ao radônio proveniente de águas subterrâneas também estaria associada ao aumento do risco de câncer pulmonar.(53)
Um estudo na Tailândia relatou diferenças significativas nos níveis residenciais de radônio entre pacientes com câncer de pulmão e controles saudáveis e estimou que 26% e 28% das mortes por câncer de pulmão em homens e mulheres, respectivamente, eram atribuíveis à exposição ao radônio em ambientes internos naquele país. Outros fatores foram identificados como capazes de interferir nos níveis internos de radônio, como as características da residência e sua ventilação. A relação janela-parede foi negativamente associada aos níveis internos de radônio.(54)
Um estudo ecológico avaliou o aumento do risco de mortalidade por câncer pulmonar causado pela exposição ao radônio em ambientes internos no México.(55) As médias das concentrações de radônio em ambientes internos variaram de 51 a 1.863 Bq/m3, a maior média de dose de exposição encontrada foi de 3,13 mSv/ano no norte do país (Chihuahua), e o excesso de mortalidade por câncer pulmonar no país foi de 10,0 ± 1,5 mortes por 105 habitantes. Os maiores valores foram encontrados no norte do país, onde existem numerosos depósitos de urânio, seguido pela Cidade do México, área mais populosa e poluída do país.(55)
Torres-Durán et al.(56) avaliaram 829 pacientes com câncer de pulmão, dos quais 56,7% eram fumantes ou ex-fumantes. Não houve associação das concentrações de radônio em ambientes internos com idade, sexo, tipo histológico ou estadiamento do tumor no momento do diagnóstico. As medianas das concentrações de radônio em ambientes internos aumentaram com a idade no momento do diagnóstico entre os homens, mas não entre as mulheres. Ao analisar os participantes expostos a mais de 1.000 Bq/m3, observou-se predomínio de câncer de pulmão de pequenas células e presença mais significativa de estágios avançados (IIIB e IV).(56)
Rodríguez-Martínez et al.(37) avaliaram, em um estudo de caso-controle multicêntrico, o efeito da exposição residencial ao radônio sobre o risco de câncer de pulmão de pequenas células na população geral. Houve associação estatisticamente significativa para os expostos a concentrações acima do permitido (OR = 2,08; IC95%: 1,03-4,39) em relação aos expostos a concentrações abaixo de 50 Bq/m3.(37)
Maggiore et al.(57) avaliaram o risco de exposição ao radônio e a incidência/mortalidade por câncer de pulmão no sudeste da Itália. No estudo em questão, os autores salientaram que o risco de exposição ao radônio deve ser mais bem estudado para avaliar as causas das taxas mais altas de mortalidade e incidência de câncer de pulmão na área de Salento em comparação com as taxas médias nacionais. Por esses motivos, a Autoridade Local de Saúde de Lecce, em cooperação com a Agência Regional de Proteção e Prevenção Ambiental da Apúlia e o Instituto de Fisiologia Clínica do Conselho Nacional de Pesquisa, incluiu o monitoramento de concentrações individuais de radônio em ambientes internos no protocolo de um estudo de caso-controle destinado a investigar o papel de diferentes fatores de risco pessoais e ambientais para câncer de pulmão na área de Salento.(57)
Segundo dados do Instituto Nacional do Câncer, o câncer de pulmão foi responsável por 28.620 mortes no Brasil em 2020, tem sido uma das principais causas de morte evitável e é, respectivamente, o terceiro e quarto tipo mais comum de câncer em homens (17.760 novos casos) e mulheres (12.440 novos casos).(58) Além disso, o câncer de pulmão é o primeiro e terceiro tipo mais comum em termos de incidência entre homens e mulheres em todo o mundo, respectivamente.(59)
O tabagismo é o fator de risco mais crítico para o desenvolvimento de câncer pulmonar. Outros fatores de risco citados pelo Instituto Nacional do Câncer, além do radônio, são exposição ocupacional a agentes químicos ou físicos (amianto, sílica, urânio, cromo, agentes alquilantes, entre outros), água potável contendo arsênico e altas doses de suplementos de beta-caroteno em fumantes e ex-fumantes. O radônio é o principal fator de câncer pulmonar em não fumantes (cerca de 10-15%, com pequenas variações).(58)
Lorenzo-González et al.(60) afirmaram que os profissionais de saúde negligenciam o radônio residencial e que ele raramente é considerado uma variável na pontuação de risco de câncer de pulmão. As discussões com jovens adultos podem ser valiosas, pois eles fazem planos de longo prazo para se estabelecerem em uma residência e no trabalho.(47) Os médicos de família desempenham um papel crucial no fornecimento de informações aos pacientes sobre os riscos da exposição ao radônio para a saúde e na recomendação de ações proativas para reduzir a exposição.(61)
Do ponto de vista clínico, quando não fumantes são diagnosticados com câncer pulmonar, o radônio deve ser considerado como potencial causa.(34,62) Do ponto de vista da saúde pública, o radônio residencial deve ser considerado um fator importante na predição do risco de câncer pulmonar, especialmente entre fumantes, em virtude do efeito sinérgico entre o radônio e a fumaça do tabaco. A cessação do tabagismo deve ser uma das principais prioridades de saúde.(34)
É necessário conscientizar os profissionais de saúde, os legisladores, os formuladores de políticas e a população para que se possa tomar as medidas necessárias para reduzir essa exposição prejudicial, particularmente em áreas propensas ao radônio, evitando assim uma proporção significativa de mortes por câncer.(63)
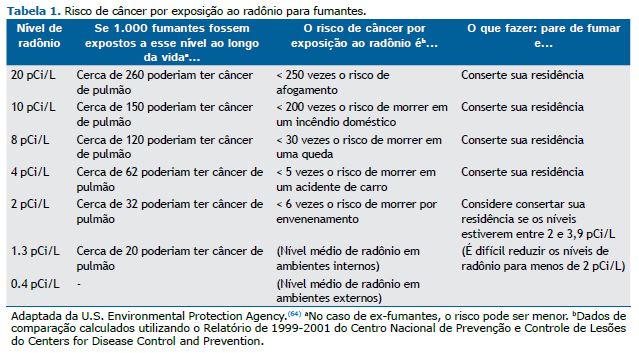
As Tabelas 1 e 2 mostram o risco de câncer pulmonar segundo o nível de exposição ao radônio e o hábito de fumar.(64)
PREVENÇÃO E MITIGAÇÃO As seguintes medidas devem ser observadas para que a exposição ao radônio tenha menor potencial destrutivo ou até mesmo não ocorra(3,65):
- Para a redução do risco na população geral, são necessárias estratégias tanto para a prevenção da liberação de radônio (em novas habitações) como para mitigação (em habitações já existentes).
- Devem ser realizadas medições periódicas de radônio para que se possa verificar a efetividade das medidas ado-tadas para prevenção e mitigação de radônio.
- Os profissionais do setor de construção são os principais atores na prevenção e mitigação da exposição ao radô-nio. Eles precisam ser treinados para garantir sua competência nessa área.
PROGRAMA IDEAL DE CONTROLE DE RADÔNIO
- A seguir estão as características e necessidades que um programa nacional de controle da exposição ao radônio deve apresentar e abordar para ser efetivo(3):
- Os programas nacionais de controle de radônio devem ter como objetivo reduzir o risco para a população geral, especialmente para os indivíduos que vivem em ambientes com altas concentrações desse gás.
- Para limitar o risco, deve ser estabelecido um nível de exposição de referência nacional de 100 Bq/m3. Caso não seja possível utilizar esse nível de referência, devem ser evitados níveis ≥ 300 Bq/m3.
- Para reduzir o risco para a população geral, devem ser implementados códigos de construção que exijam medi-ções de radônio nas casas em construção.
- As medições de radônio são necessárias porque os códigos de construção por si só não podem garantir que as concentrações estarão abaixo do nível de referência.
- Um programa nacional efetivo de controle de radônio requer a contribuição de múltiplas agências do mesmo país. Uma agência deve liderar a implementação e coordenação e garantir a ligação com o controle do tabaco, e uma deve liderar os programas de promoção da saúde.
EXEMPLOS DE AÇÕES Plano Nacional de Ação contra o Radônio — 2021-2025 Os objetivos do Plano Nacional de Ação contra o Radônio — 2021-2025 dos EUA(66) são encontrar, corrigir e evitar níveis elevados de radônio em oito milhões de edifícios até 2025 e evitar 3.500 mortes por câncer de pulmão anualmente. No âmbito desse plano, líderes de diversos setores trabalham em conjunto para planejar, orientar e sustentar ações nacionais para a prevenção da exposição ao radônio(66):
- Eliminar o câncer de pulmão evitável causado pelo radônio, por meio da ampliação das proteções para todas as comunidades e edifícios.
- A única maneira de determinar os níveis de radônio em ambientes internos é por meio de testes.
- Profissionais qualificados podem instalar um sistema que informa quando altos níveis de radônio estão se acumu-lando no interior do edifício.
- Os novos edifícios devem ser projetados e construídos utilizando técnicas de construção resistentes ao radônio, a fim de salvar vidas agora e no futuro.
- Como é menor a probabilidade de que indivíduos e famílias de baixa renda testem os níveis de radônio de suas residências, é necessária a conscientização do governo sobre esse tipo de problema.
- Algumas pessoas não sabem que a exposição ao radônio em ambientes internos pode causar câncer de pulmão; assim, há uma necessidade urgente de mais divulgação. g. Alguns inquilinos, ou mesmo proprietários, po-dem contestar essas disposições para a proteção das residências por não conseguirem arcar com os custos de testes e mitigação de radônio.
- Como se espera que a redução das altas concentrações de radônio em residências e outros edifícios resulte em importantes benefícios para a saúde, o acesso a proteções que salvam vidas contra o radônio deve ser mais equitativo entre os grupos sociais.
NOVA REGULAMENTAÇÃO ESPANHOLA PARA PROTEÇÃO CONTRA A EXPOSIÇÃO AO RADÔNIO O Real Decreto espanhol n. 1029/2022, de 20 de dezembro de 2022, estabelece que o nível de referência para a concentração de radônio em áreas internas é de 300 Bq/m3 em termos da concentração média anual de radônio no ar em residências, edifícios de acesso público e locais de trabalho.(67)
A nova regulamentação espanhola estabelece a obrigação de realizar medições de radônio em todos os edifícios de acesso público, comércios, empresas e residências, especialmente em áreas com altos níveis de radônio. Se forem detectados altos níveis desse gás, devem ser tomadas medidas para reduzir e mitigar a exposição (instalação de sistemas de redução de radônio, por exemplo).(67)
CONSIDERAÇÕES FINAIS Segundo Stanifer et al.,(68) o teste de radônio residencial é uma estratégia de prevenção primária do câncer de pulmão. Áreas com alta prevalência de tabagismo em adultos e alta incidência de câncer de pulmão podem se beneficiar mais de intervenções de prevenção voltadas à promoção do teste de radônio residencial, à adoção de políticas de residências livres de radônio e de tabagismo e à integração de mensagens de redução dos riscos do radônio em programas de cessação do tabagismo e de triagem do câncer de pulmão.
Os principais passos para reduzir as mortes por câncer de pulmão induzidas pela exposição ao radônio são aumentar a conscientização do público e dos profissionais de saúde sobre essa ameaça, medir os níveis de radônio em todos os tipos de edifícios novos, construir uma força de trabalho de profissionais qualificados que possam resolver problemas relacionados ao radônio utilizando padrões comprovados e garantir que haja financiamento adequado disponível para cobrir os custos de testes e reparos.
CONTRIBUIÇÕES DOS AUTORES Todos os autores contribuíram igualmente para este trabalho e aprovaram a versão final do manuscrito.
CONFLITOS DE INTERESSE Nenhum declarado.
REFERÊNCIAS 1. Shakoor H, Jehan N, Khan S, Khattak NU. Investigation of Radon Sources, Health Hazard and Risks assessment for children using analytical and geospatial techniques in District Bannu (Pakistan). Int J Radiat Biol. 2022;98(6):1176-1184. https://doi.org/10.1080/09553002.2021.1872817
2. Ngoc LTN, Park D, Lee YC. Human Health Impacts of Residential Radon Exposure: Updated Systematic Review and Meta-Analysis of Case-Control Studies. Int J Environ Res Public Health. 2022;20(1):97. https://doi.org/10.3390/ijerph20010097
3. Zeeb H, Shannoun F, editors. Manual da OMS sobre radônio em ambientes internos: uma perspectiva de saúde. 1st Ed; 2016. [Adobe Acrobat document, 122p.]. Available from: https://www.gov.br/ird/pt-br/central-de-conteudo/publicacoes/ManualdaOMSsobreradonioemambientesinternos.pdf
4. Gawande S, Tiwari RR, Narayanan P, Bhadri A. Indoor Air Quality and Sick Building Syndrome: Are Green Buildings Better than Conventional Buildings?. Indian J Occup Environ Med. 2020;24(1):30-32. https://doi.org/10.4103/ijoem.IJOEM_148_19
5. Nunes LJR, Curado A, Graça LCCD, Soares S, Lopes SI. Impacts of Indoor Radon on Health: A Comprehensive Review on Causes, Assessment and Remediation Strategies. Int J Environ Res Public Health. 2022;19(7):3929. https://doi.org/10.3390/ijerph19073929
6. Chapter 42. Radon. In: Etzel RA, Balk SJ, editors. Pediatric Environmental Health. 4th ed. Itasca, IL: American Academy of Pediatrics; 2018. p.739-746.
7. U.S. Environmental Protection Agency (EPA) [homepage on the Internet]. Washington, DC: EPA; c2023 [cited 2023 Feb 1]. Available from: https://www.epa.gov
8. Corrales L, Rosell R, Cardona AF, Martín C, Zatarain-Barrón ZL, Arrieta O. Lung cancer in never smokers: The role of different risk factors other than tobacco smoking. Crit Rev Oncol Hematol. 2020;148:102895. https://doi.org/10.1016/j.critrevonc.2020.102895
9. International Commission on Radiological Protection (ICRP) [homepage on the Internet]. Ottawa, ON: ICRP; c2023 [updated 2014; cited 2023 Mar 1]. Radiological Protection against Radon Exposure. Available from: https://www.icrp.org/publication.asp?id=ICRP%20Publication%20126
10. Brasil. Ministério da Saúde. Instituto Nacional do Câncer (INCA) [homepage on the Internet]. Rio de Janeiro: INCA. Projeto Planalto de Poços de Caldas: Pesquisa câncer e radiação natural: Minas Gerais-Brasil: 2004 a 2009, vol.1. Belo Horizonte: SES-MG; 2009. Available from: https://www.inca.gov.br/publicacoes/livros/projeto-planalto-pocos-de-caldas-pesquisa-cancer-e-radiacao-natural
11. Antoniazzi BN, Silva NC, Cunha TN, Otero UB. Projeto Planalto de Poços de Caldas: Pesquisa câncer e radiação natural: incidência e comportamento de risco: Minas Gerais - Brasil 2004 a 2013. Belo Horizonte: SES-MG; 2013.
12. Fianco ACB. Concentrações de randônio nas águas subterrâneas, rochas e solos de Porto Alegre, RS [dissertation]. Porto Alegre: Universidade Federal do Rio Grande do Sul; 2011. 99p. Available from: https://lume.ufrgs.br/handle/10183/32667
13. Lopes SI, Nunes LJR, Curado A. Designing an Indoor Radon Risk Exposure Indicator (IRREI): An Evaluation Tool for Risk Management and Communication in the IoT Age. Int J Environ Res Public Health. 2021;18(15):7907. https://doi.org/10.3390/ijerph18157907
14. Chen J. RISK ASSESSMENT FOR RADON EXPOSURE IN VARIOUS INDOOR ENVIRONMENTS. Radiat Prot Dosimetry. 2019;185(2):143-150. https://doi.org/10.1093/rpd/ncy284
15. Baloch RM, Maesano CN, Christoffersen J, Banerjee S, Gabriel M, Csobod É, et al. Indoor air pollution, physical and comfort parameters related to schoolchildren’s health: Data from the European SINPHONIE study. Sci Total Environ. 2020;739:139870. https://doi.org/10.1016/j.scitotenv.2020.139870
16. Zhukovsky M, Vasilyev A, Onishchenko A, Yarmoshenko I. REVIEW OF INDOOR RADON CONCENTRATIONS IN SCHOOLS AND KINDERGARTENS. Radiat Prot Dosimetry. 2018;181(1):6-10. https://doi.org/10.1093/rpd/ncy092
17. Davis EA, Ou JY, Chausow C, Verdeja MA, Divver E, Johnston JD, et al. Associations Between School Characteristics and Classroom Radon Concentrations in Utah’s Public Schools: A Project Completed by University Environmental Health Students. Int J Environ Res Public Health. 2020;17(16):5839. https://doi.org/10.3390/ijerph17165839
18. Branco PT, Nunes RA, Alvim-Ferraz MC, Martins FG, Sousa SI. Children’s Exposure to Radon in Nursery and Primary Schools. Int J Environ Res Public Health. 2016;13(4):386. https://doi.org/10.3390/ijerph13040386
19. Curado A, Silva JP, Lopes SI. Radon risk assessment in a low energy consumption school building: A dosimetric approach for effective risk management. Energy Rep. 2020;6(Suppl 1):897-902. 10.1016/j.egyr.2019.11.155 https://doi.org/10.1016/j.egyr.2019.11.155
20. Sabbarese C, Ambrosino F, D’Onofrio A. Development of radon transport model in different types of dwellings to assess indoor activity concentration. J Environ Radioact. 2021;227:106501. https://doi.org/10.1016/j.jenvrad.2020.106501
21. Khan SM, Pearson DD, Rönnqvist T, Nielsen ME, Taron JM, Goodarzi AA. Rising Canadian and falling Swedish radon gas exposure as a consequence of 20th to 21st century residential build practices. Sci Rep. 2021;11(1):17551. https://doi.org/10.1038/s41598-021-96928-x
22. Shergill S, Forsman-Phillips L, Nicol AM. Radon in Schools: A Review of Radon Testing Efforts in Canadian Schools. Int J Environ Res Public Health. 2021;18(10):5469. https://doi.org/10.3390/ijerph18105469
23. Taylor BK, Smith OV, Miller GE. Chronic Home Radon Exposure Is Associated with Higher Inflammatory Biomarker Concentrations in Children and Adolescents. Int J Environ Res Public Health. 2022;20(1):246. https://doi.org/10.3390/ijerph20010246
24. Simms JA, Pearson DD, Cholowsky NL, Irvine JL, Nielsen ME, Jacques WR, et al. Younger North Americans are exposed to more radon gas due to occupancy biases within the residential built environment. Sci Rep. 2021;11(1):6724. https://doi.org/10.1038/s41598-021-86096-3
25. Ramos MOS. Radônio-222 e a Ocorrência de Câncer de Pulmão em Municípios da Região Metropolitana de Recife com Afloramentos de Fosforito Uranífero [thesis]. -Recife: Universidade Federal de Pernambuco; 2020.
26. Petroni R, Lima SC. Os perigos associados a concentração de radônio (222Rn) em ambientes climatizados. Conforlab Engenharia Ambiental. Available from: https://conforlab.com.br
27. Huntington-Moskos L, Rayens MK, Wiggins A, Hahn EJ. Radon, Secondhand Smoke, and Children in the Home: Creating a Teachable Moment for Lung Cancer Prevention. Public Health Nurs. 2016;33(6):529-538. https://doi.org/10.1111/phn.12283
28. Neri A, McNaughton C, Momin B, Puckett M, Gallaway MS. Measuring public knowledge, attitudes, and behaviors related to radon to inform cancer control activities and practices. Indoor Air. 2018;28(4):604-610. https://doi.org/10.1111/ina.12468
29. Riudavets M, Garcia de Herreros M, Besse B, Mezquita L. Radon and Lung Cancer: Current Trends and Future Perspectives. Cancers (Basel). 2022;14(13):3142. https://doi.org/10.3390/cancers14133142
30. Kang JK, Seo S, Jin YW. Health Effects of Radon Exposure. Yonsei Med J. 2019;60(7):597-603. https://doi.org/10.3349/ymj.2019.60.7.597
31. Ruano-Ravina A, Varela Lema L, García Talavera M, García Gómez M, González Muñoz S, Santiago-Pérez MI, et al. Lung cancer mortality attributable to residential radon exposure in Spain and its regions. Environ Res. 2021;199:111372. https://doi.org/10.1016/j.envres.2021.111372
32. Thandra KC, Barsouk A, Saginala K, Aluru JS, Barsouk A. Epidemiology of lung cancer. Contemp Oncol (Pozn). 2021;25(1):45-52. https://doi.org/10.5114/wo.2021.103829
33. Reddy A, Conde C, Peterson C, Nugent K. Residential radon exposure and cancer. Oncol Rev. 2022;16(1):558. https://doi.org/10.4081/oncol.2022.558
34. Cheng ES, Egger S, Hughes S, Weber M, Steinberg J, Rahman B, et al. Systematic review and meta-analysis of residential radon and lung cancer in never-smokers. Eur Respir Rev. 2021;30(159):200230. https://doi.org/10.1183/16000617.0230-2020
35. Robertson A, Allen J, Laney R, Curnow A. The cellular and molecular carcinogenic effects of radon exposure: a review. Int J Mol Sci. 2013;14(7):14024-14063. https://doi.org/10.3390/ijms140714024
36. Barros-Dios JM, Ruano-Ravina A, Pérez-Ríos M, Castro-Bernárdez M, Abal-Arca J, Tojo-Castro M. Residential radon exposure, histologic types, and lung cancer risk. A case-control study in Galicia, Spain. Cancer Epidemiol Biomarkers Prev. 2012;21(6):951-958. https://doi.org/10.1158/1055-9965.EPI-12-0146-T
37. Rodríguez-Martínez Á, Ruano-Ravina A, Torres-Durán M, Provencio M, Parente-Lamelas I, Vidal-García I, et al. Residential Radon and Small Cell Lung Cancer. Final Results of the Small Cell Study. Arch Bronconeumol. 2022;58(7):542-546. https://doi.org/10.1016/j.arbres.2021.01.027
38. Krewski D, Lubin JH, Zielinski JM, Alavanja M, Catalan VS, Field RW, et al. Residential radon and risk of lung cancer: a combined analysis of 7 North American case-control studies. Epidemiology. 2005;16(2):137-145. https://doi.org/10.1097/01.ede.0000152522.80261.e3
39. Zhang ZL, Sun J, Dong JY, Tian HL, Xue L, Qin LQ, et al. Residential radon and lung cancer risk: an updated meta- analysis of case-control studies. Asian Pac J Cancer Prev. 2012;13(6):2459-2465. https://doi.org/10.7314/APJCP.2012.13.6.2459
40. Darby S, Hill D, Deo H, Auvinen A, Barros-Dios JM, Baysson H, et al. Residential radon and lung cancer--detailed results of a collaborative analysis of individual data on 7148 persons with lung cancer and 14,208 persons without lung cancer from 13 epidemiologic studies in Europe [published correction appears in Scand J Work Environ Health. 2007 Feb;33(1):80]. Scand J Work Environ Health. 2006;32 Suppl 1:1-83.
41. Leuraud K, Schnelzer M, Tomasek L, Hunter N, Timarche M, Grosche B, et al. Radon, smoking and lung cancer risk: results of a joint analysis of three European case-control studies among uranium miners. Radiat Res. 2011;176(3):375-387. https://doi.org/10.1667/RR2377.1
42. Dubin S, Griffin D. Lung Cancer in Non-Smokers. Mo Med. 2020;117(4):375-379.
43. Darby S, Hill D, Auvinen A, Barros-Dios JM, Baysson H, Bochicchio F, et al. Radon in homes and risk of lung cancer: collaborative analysis of individual data from 13 European case-control studies. BMJ. 2005;330(7485):223. https://doi.org/10.1136/bmj.38308.477650.63
44. Lorenzo-Gonzalez M, Ruano-Ravina A, Torres-Duran M, Kelsey KT, Provencio M, Parente-Lamelas I, et al. Lung cancer risk and residential radon exposure: A pooling of case-control studies in northwestern Spain. Environ Res. 2020;189:109968. https://doi.org/10.1016/j.envres.2020.109968
45. Su C, Pan M, Liu N, Zhang Y, Kan H, Zhao Z, et al. Lung cancer as adverse health effect by indoor radon exposure in China from 2000 to 2020: A systematic review and meta-analysis. Indoor Air. 2022;32(11):e13154. https://doi.org/10.1111/ina.13154
46. Li C, Wang C, Yu J, Fan Y, Liu D, Zhou W, et al. Residential Radon and Histological Types of Lung Cancer: A Meta-Analysis of Case-Control Studies. Int J Environ Res Public Health. 2020;17(4):1457. https://doi.org/10.3390/ijerph17041457
47. Mema SC, Baytalan G. Radon and lung cancer risk. CMAJ. 2023;195(24):E850. https://doi.org/10.1503/cmaj.230110
48. MitigAir [homepage on the Internet]. Ottawa: Health Canada; 2021 [cited 2023 Jul 1]. Radon - what you need to know. Available from: https://www.mitigair.com/?gclid=Cj0KCQjwk96lBhDHARIsAEKO4xaCBSksmnEahL8pga2yXcqu_cregLx_KBAm4FoBdk2lFSSCqPbQF84aAl8dEALw_wcB
49. Khan SM, Pearson DD, Rönnqvist T, Nielsen ME, Taron JM, Goodarzi AA. Rising Canadian and falling Swedish radon gas exposure as a consequence of 20th to 21st century residential build practices. Sci Rep. 2021;11(1):17551. https://doi.org/10.1038/s41598-021-96928-x
50. Government of Canada [homepage on the Internet]. Ottawa: Health Canada; c2019 [cited 2023 Jul 1]. Radon: Is it in your home? Information for health professionals. Available from: https://www.canada.ca/en/health-canada/services/environmental-workplace-health/reports-publications/radiation/radon-is-it-in-you-home-information-health-professionals.html
51. Messier KP, Serre ML. Lung and stomach cancer associations with groundwater radon in North Carolina, USA. Int J Epidemiol. 2017;46(2):676-685. https://doi.org/10.1093/ije/dyw128
52. Kurkela O, Nevalainen J, Pätsi SM, Kojo K, Holmgren O, Auvinen A. Lung cancer incidence attributable to residential radon exposure in Finland. Radiat Environ Biophys. 2023;62(1):35-49. https://doi.org/10.1007/s00411-022-01004-1
53. Hadkhale K, Atosuo J, Putus T. Groundwater radon exposure and risk of lung cancer: A population-based study in Finland. Front Oncol. 2022;12:935687. https://doi.org/10.3389/fonc.2022.935687
54. Somsunun K, Prapamontol T, Pothirat C, Liwsrisakun C, Pongnikorn D, Fongmoon D, et al. Estimation of lung cancer deaths attributable to indoor radon exposure in upper northern Thailand. Sci Rep. 2022;12(1):5169. https://doi.org/10.1038/s41598-022-09122-y
55. Ponciano-Rodríguez G, Gaso MI, Armienta MA, Trueta C, Morales I, Alfaro R, et al. Indoor radon exposure and excess of lung cancer mortality: the case of Mexico-an ecological study. Environ Geochem Health. 2021;43(1):221-234. https://doi.org/10.1007/s10653-020-00662-8
56. Torres-Durán M, Casal-Mouriño A, Ruano-Ravina A, Provencio M, Parente-Lamelas I, Hernández-Hernández J, et al. Residential radon and lung cancer characteristics at diagnosis. Int J Radiat Biol. 2021;97(7):997-1002. https://doi.org/10.1080/09553002.2021.1913527
57. Maggiore G, DE Filippis G, Totaro T, Tamborino B, Idolo A, Serio F, et al. Evaluation of radon exposure risk and lung cancer incidence/mortality in South-eastern Italy. J Prev Med Hyg. 2020;61(1):E31-E38.
58. Brasil. Ministério da Saúde. Instituto Nacional do Câncer (INCA) [homepage on the Internet]. Rio de Janeiro: INCA; c2022 [updated 2022 Jul 18; cited 2023 Feb 1]. Câncer de Pulmão. Available from: https://www.gov.br/inca/pt-br/assuntos/cancer/tipos/pulmao
59. Huang J, Deng Y, Tin MS, Lok V, Ngai CH, Zhang L, et al. Distribution, Risk Factors, and Temporal Trends for Lung Cancer Incidence and Mortality: A Global Analysis. Chest. 2022;161(4):1101-1111. https://doi.org/10.1016/j.chest.2021.12.655
60. Lorenzo-González M, Torres-Durán M, Barbosa-Lorenzo R, Provencio-Pulla M, Barros-Dios JM, Ruano-Ravina A. Radon exposure: a major cause of lung cancer. Expert Rev Respir Med. 2019;13(9):839-850. https://doi.org/10.1080/17476348.2019.1645599
61. Field RW. Radon: A Leading Environmental Cause of Lung Cancer. Am Fam Physician. 2018;98(5):280-282.
62. Ruano-Ravina A, Fernández-Villar A, Barros-Dios JM. Residential Radon and Risk of Lung Cancer in Never-Smokers. Arch Bronconeumol. 2017;53(9):475-476. https://doi.org/10.1016/j.arbres.2017.01.004
63. Gaskin J, Coyle D, Whyte J, Krewksi D. Global Estimate of Lung Cancer Mortality Attributable to Residential Radon. Environ Health Perspect. 2018;126(5):057009. https://doi.org/10.1289/EHP2503
64. U.S. Environmental Protection Agency (EPA) [homepage on the Internet]. Washington, DC: EPA; A Citizen’s Guide to Radon: the Guide TO Protecting Yourself and Your Family from Radon; 2016. Available from: https://www.epa.gov/sites/default/files/2016-12/documents/2016_a_citizens_guide_to_radon.pdf
65. Khan SM, Gomes J, Krewski DR. Radon interventions around the globe: A systematic review. Heliyon. 2019;5(5):e01737. https://doi.org/10.1016/j.heliyon.2019.e01737
66. Radonleaders.org [homepage on the Internet]; c2022 [updated 2022 Jan; cited 2023 Feb 1]. The National Radon Action Plan 2021-2025. Available from: http://www.radonleaders.org/sites/default/files/2022-01/NRAP-2021-2025-Action-Plan-508.pdf
67. Instituto para la Salud Geoambiental [homepage on the Internet]. Madrid: Instituto para la Salud Geoambiental; c2022 [cited 2023 Feb 1]. Nueva ley de protección frente al radón. Disponível em: https://www.saludgeoambiental.org/nueva-ley-de-proteccion-frente-al-rado
68. Stanifer SR, Rayens MK, Wiggins A, Hahn EJ. Social Determinants of Health, Environ-mental Exposures and Home Radon Testing. West J Nurs Res. 2022;44(7):636-642. https://doi.org/10.1177/01939459211009561













 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket