CONTEXTO Definir se resultados de testes de função pulmonar (TFP) estão fora da faixa esperada tem implicações diagnósticas óbvias. Muitos médicos consideram que qualquer valor fora de ± 20% do previsto ou uma VEF1/CVF < 0,7 indica anormalidade. As diretrizes atuais apoiam fortemente o uso dos “limites” estatísticos “de normalidade” para classificar os resultados dos testes como baixos — menor que o limite inferior de normalidade (LIN) — ou elevados — maior que o limite superior de normalidade (LSN).(1) Isso realmente importa? Em caso afirmativo, podemos utilizar com segurança os critérios LIN/LSN gerais em populações clínicas?
PANORAMA A Tabela 1A mostra que o percentil 5 para VEF1 e CVF é sistematicamente maior que 80% do previsto em homens e mulheres mais jovens (LIN > 0,7 para VEF1/CVF), e o oposto é observado em idosos. Por outro lado, o LIN para volumes pulmonares “estáticos” e DLCO é tipicamente menor que 80%, independentemente da idade e do sexo. A Tabela 1B mostra os resultados espirométricos de uma jovem não fumante com sobrepeso que relatou episódios recorrentes de dispneia: 0,7 < VEF1/CVF < LIN sugeriu defeito ventilatório obstrutivo. A Tabela 1C mostra os resultados espirométricos de uma idosa ex-fumante que relatou dispneia crônica e tosse produtiva. Seus sintomas, a presença de espessamento de parede brônquica na TC de tórax e relação VEF1/CVF < 0,7, apesar de essa última estar acima do LIN, foram considerados consistentes com obstrução. Ambas as pacientes relataram melhora acentuada com o uso de formoterol/budesonida inalatórios.
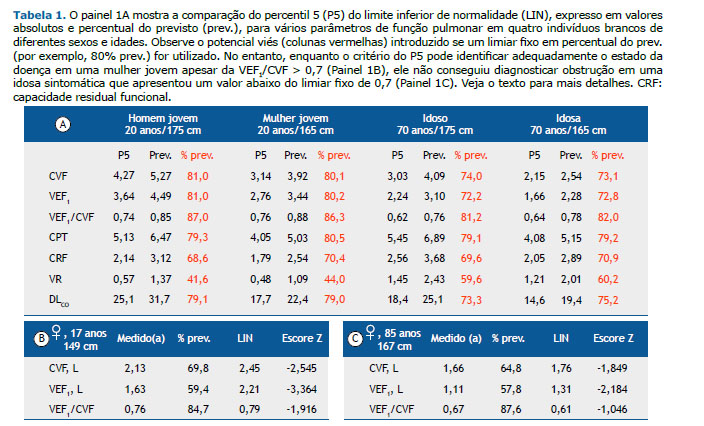
Nossa incerteza sobre o que constitui VEF1, CVF e VEF1/CVF normais aumenta com o envelhecimento, ou seja, o LIN está longe dos valores previstos em idosos (Tabela 1A). Assim, valores < 80% do previsto podem estar bem dentro da faixa esperada nos idosos, mas anormais nos jovens. A adesão rígida ao limiar de 80% ou 120% do previsto é ainda mais problemática para os volumes pulmonares, aumentando acentuadamente a taxa de falso-positivos (Tabela 1A). Isso não implica que os limites estatísticos de normalidade sejam imunes a erros. O melhor exemplo é o limiar do LIN para VEF1/CVF: até um terço dos idosos em risco de DPOC com LIN < VEF1/CVF < 0,7 apresentaram uma variedade de anormalidades em repouso e durante o exercício consistentes com DPOC. (2) De fato, variações mínimas no valor de corte para definir o limiar de normalidade para VEF1/CVF têm um impacto acentuado no percentual de todos os casos em toda a população que pode ser atribuído à exposição (tabagismo). Isso é particularmente verdadeiro em idosos, pois, conforme mencionado, a variabilidade é maior; assim, uma fração considerável de pacientes com DPOC apresentará VEF1/CVF “preservada”, ou seja, acima do percentil 5 (Tabela 1C).(3) Em muitas circunstâncias, valores dentro da “zona cinza” (por exemplo, entre 80% do previsto e LIN; 120% do previsto e LSN; ou LIN < VEF1/CVF < 0,7) devem ser interpretados individualmente à luz da probabilidade pré-teste de anormalidade.(4)
MENSAGEM CLÍNICA O uso de limiares fixos (como 80% ou 120% do previsto) para classificar resultados de TFP como anormais pode levar a erros substanciais, geralmente resultando em “subestimação” de doença nos jovens e “superestimação” de doença nos idosos. O LIN estatístico, no entanto, está longe de ser uma panaceia: a interpretação dos TFP será sempre um N = 1 estudo, exigindo correlação clínica cuidadosa para julgar a normalidade dos valores próximos do limiar proposto.(5)
REFERÊNCIAS 1. Stanojevic S, Kaminsky DA, Miller M, Thompson B, Aliverti A, Barjaktarevic I, et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J. 2021;2101499. https://doi.org/10.1183/13993003.01499-2021
2. Neder JA, Milne KM, Berton DC, de-Torres JP, Jensen D, Tan WC, et al. Exercise Tolerance according to the Definition of Airflow Obstruction in Smokers. Am J Respir Crit Care Med. 2020;202(5):760-762. https://doi.org/10.1164/rccm.202002-0298LE
3. Burney P, Minelli C. Using reference values to define disease based on the lower limit of normal biased the population attributable fraction, but not the population excess risk: the example of chronic airflow obstruction. J Clin Epidemiol. 2018;93:76-78. https://doi.org/10.1016/j.jclinepi.2017.10.020
4. Neder JA, Berton DC, O’Donnell DE. The Lung Function Laboratory to Assist Clinical Decision-making in Pulmonology: Evolving Challenges to an Old Issue. Chest. 2020;158(4):1629-1643. https://doi.org/10.1016/j.chest.2020.04.064
5. Neder JA. Functional respiratory assessment: some key misconceptions and their cli-nical implications. Thorax. 2021;76(7):644-646. https://doi.org/10.1136/thoraxjnl-2020-215287






 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket




