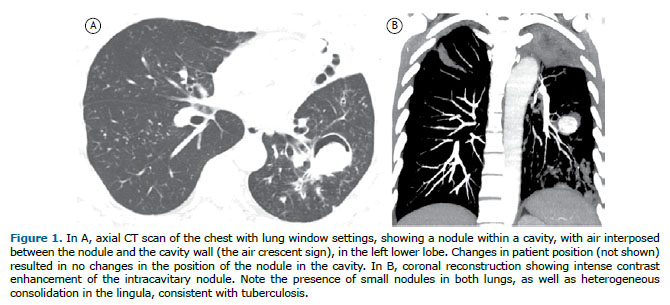
A 40-year-old man presented with a 3-month history of cough, fever, and weight loss, progressing to an episode of hemoptysis. A CT scan of the chest showed an intensely enhanced intracavitary nodule, with air interposed between the nodule and the cavity wall (the air crescent sign - ACS - Figure 1).
The ACS is a crescent– or half-moon–shaped collection of air in the periphery of an intracavitary nodule or mass, separating the nodule or mass from the cavity wall. The finding of a nodule in a lung cavity has important diagnostic and therapeutic implications. The most common cause of an ACS is a fungus ball, or aspergilloma, resulting from Aspergillus colonization of preexisting lung cavities. However, the ACS has been reported in association with a variety of lung diseases, including neoplasms (particularly bronchial carcinoma), recovery from angioinvasive aspergillosis, Rasmussen’s aneurysm, and intracavitary clots. Other, rarer, causes include foreign bodies, thick pus, dehydrated caseous material, teratoma, and hydatid disease.(1,2)
A change in the position of the nodule in the cavity when patient position is changed, especially during CT examinations in the supine and prone positions, can be useful in the differential diagnosis. It is extremely important to determine whether the central mass is free or attached to the cavity wall because, unlike a fungus ball or a clot, cavitary lung cancer and Rasmussen’s aneurysm present as masses that are fixed to the cavity wall; that is, they do not move when patient position is changed. Intense contrast enhancement of the nodule is seen in Rasmussen’s aneurysm and can be useful in the differential diagnosis with aspergilloma, in which it is not.(1,2)
In the case reported here, the final diagnosis was Rasmussen’s aneurysm in a patient with active tuberculosis. Rasmussen’s aneurysms are pulmonary artery pseudoaneurysms secondary to pulmonary tuberculosis. In patients with Rasmussen’s aneurysm, as well as in those with aspergilloma, hemoptysis is a common initial manifestation and can be fatal when massive. In conclusion, although aspergilloma is the most common cause of intracavitary nodules, other conditions should be considered in the differential diagnosis, including intracavitary tumors and Rasmussen’s aneurysm. An accurate diagnosis is crucial and can have implications for disease management and prognosis.
REFERENCES 1. Marchiori E, Hochhegger B, Zanetti G. Intracavitary nodule. J Bras Pneumol. 2016;42(5):309. https://doi.org/10.1590/S1806-37562016000000223
2. Sevilha JB, Rodrigues RS, Barreto MM, Zanetti G, Hochhegger B, Marchiori E. Infectious and Non-Infectious Diseases Causing the Air Crescent Sign: A State-of-the-Art Review. Lung. 2018;196(1):1-10. https://doi.org/10.1007/s00408-017-0069-3






 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket




