ABSTRACT
Objective: To present official longitudinal data on the impact of asthma in Brazil between 2008 and 2013. Methods: This was a descriptive study of data collected between 2008 and 2013 from an official Brazilian national database, including data on asthma-related number of hospitalizations, mortality, and hospitalization costs. A geographical subanalysis was also performed. Results: In 2013, 2,047 people died from asthma in Brazil (5 deaths/day), with more than 120,000 asthma-related hospitalizations. During the whole study period, the absolute number of asthma-related deaths and of hospitalizations decreased by 10% and 36%, respectively. However, the in-hospital mortality rate increased by approximately 25% in that period. The geographic subanalysis showed that the northern/northeastern and southeastern regions had the highest asthma-related hospitalization and in-hospital mortality rates, respectively. An analysis of the states representative of the regions of Brazil revealed discrepancies between the numbers of asthma-related hospitalizations and asthma-related in-hospital mortality rates. During the study period, the cost of asthma-related hospitalizations to the public health care system was US$ 170 million. Conclusions: Although the numbers of asthma-related deaths and hospital admissions in Brazil have been decreasing since 2009, the absolute numbers are still high, resulting in elevated direct and indirect costs for the society. This shows the relevance of the burden of asthma in middle-income countries.
Keywords:
Asthma/epidemiology; Asthma/mortality; Public health; Hospitalization.
RESUMO
Objetivo: Apresentar dados longitudinais oficiais sobre o impacto da asma no Brasil entre 2008 e 2013. Métodos: Estudo descritivo de dados extraídos de um banco de dados do governo brasileiro entre 2008 e 2013, no qual foram analisados as hospitalizações e óbitos por asma, bem como o custo das hospitalizações. Foi também realizada uma subanálise geográfica. Resultados: Em 2013, 2.047 pessoas morreram de asma no Brasil (5 óbitos/dia), com mais de 120.000 hospitalizações por asma. Durante o período de estudo, o número absoluto de óbitos e hospitalizações por asma diminuiu 10% e 36%, respectivamente. No entanto, a taxa de mortalidade hospitalar aumentou aproximadamente 25%. A subanálise geográfica mostrou que as regiões Norte/Nordeste e Sudeste apresentaram as maiores taxas de hospitalização e mortalidade hospitalar por asma, respectivamente. A análise dos estados representativos de cada região mostrou discrepâncias entre as hospitalizações por asma e as taxas de mortalidade hospitalar por asma. Durante o período de estudo, as hospitalizações por asma custaram US$ 170 milhões ao sistema público de saúde. Conclusões: Embora os óbitos e hospitalizações por asma no Brasil estejam diminuindo desde 2009, os números absolutos ainda são altos, com elevados custos diretos e indiretos para a sociedade, o que mostra a relevância do impacto da asma em países de renda média.
Palavras-chave:
Asma/epidemiologia; Asma/mortalidade; Saúde pública; Hospitalização.
INTRODUÇÃOA asma é uma doença crônica tratável das vias aéreas que afeta todas as faixas etárias e apresenta alta prevalência, morbidade e mortalidade em todo o mundo. (1,2) Vários pacientes vivem com asma não controlada, que, além de prejudicar a qualidade de vida, resulta em custos diretos e indiretos à sociedade, particularmente em países em desenvolvimento.(3-5) A prevalência da asma (inclusive a da asma grave) é alta em vários países, com impacto relevante na saúde pública global. (6,7) As populações com maior prevalência de asma (> 20% em crianças) estão em países de língua inglesa e na América Latina.(8)
A prevalência da asma infantil na América Latina varia muito (de 4% a 30%), mas está acima de 10% em praticamente todos os países.(9-12) O impacto da asma nesses países é geralmente complicada pelo acesso limitado aos serviços de saúde e medicamentos essenciais.(4,8,13) O Brasil, país de renda média de tamanho continental, é um dos países com maior prevalência de asma em crianças, com altas taxas de asma grave.(6,7,14) Mostramos recentemente que, no sul do Brasil, 20% das crianças em idade escolar têm asma, muitas delas com doença não controlada e altas taxas de inatividade física, absenteísmo escolar e hospitalizações.(15) No entanto, há poucos dados nacionais sobre o impacto da asma em países em desenvolvimento. Dados sobre a mortalidade e o número de hospitalizações referentes a uma determinada doença são importantes para orientar as políticas públicas de saúde. Grandes bancos de dados nacionais são incomuns em países em desenvolvimento. No entanto, quando disponíveis, dados desse tipo fornecem informações valiosas para melhorar as políticas de saúde para doenças prevalentes.
O Brasil possui um banco de dados oficial e longitudinal de acesso livre do Sistema Único de Saúde, que registra indicadores de saúde como taxas de mortalidade e número/custo de hospitalizações.(16) Assim, o objetivo de nosso estudo foi apresentar dados longitudinais sobre o impacto da asma no Brasil nos últimos anos e analisar fatores geográficos a respeito da doença.
MÉTODOSTrata-se de um estudo descritivo baseado em informações sobre a asma extraídas do banco de dados do Departamento de Informática do Sistema Único de Saúde (DATASUS).(16) A população estudada consistiu em todos os casos de asma - conforme a definição da Classificação Internacional de Doenças, 10ª revisão (CID-10; código J45) - em que hospitalizações e óbitos foram relatados entre 2008 e 2013. Para a análise geográfica, as variáveis foram corrigidas pelo número populacional em 2010, de acordo com regiões e estados, por meio de outro banco de dados: o banco de dados do Instituto Brasileiro de Geografia e Estatística (IBGE), que fornece dados sobre a população brasileira por meio de censos periódicos.(17) Os gráficos foram preparados com o programa estatístico GraphPad Prism, versão 6 (GraphPad Inc., San Diego, CA, EUA). Como o banco de dados do DATASUS é de domínio público, não foi necessário obter a aprovação de nosso comitê de ética em pesquisa.
Os dados extraídos do banco de dados do DATASUS foram subdivididos em três grupos para análise: Brasil, regiões e estados. Foram analisadas as seguintes variáveis: número de óbitos, número de hospitalizações, tempo de hospitalização e custos financeiros da hospitalização.
Para a análise geral, nossa pesquisa foi realizada de 2008 a 2013, por meio da ferramenta Sistema de Informação de Saúde. Para as variáveis analisadas, foram usadas as tabelas de Epidemiologia e Morbidade do grupo "Morbidade Hospitalar" e, em seguida, o subitem "Geral, por localização hospitalar". Nas opções de filtro, os itens "anos", "conteúdo das hospitalizações", "média de tempo de hospitalização", "custo total", "média de custo da hospitalização" e "óbitos" foram selecionados e correlacionados com "asma" (código J45 na CID-10). Os dados referentes ao total de óbitos, com o objetivo de cobrir todos os casos de óbitos relacionados com a asma e não apenas aqueles relacionados com as hospitalizações, foram extraídos do Sistema de Informação sobre Mortalidade por meio do item "Estatísticas Vitais" (Grupo de Mortalidade, 1996 a 2014) e do subitem "Mortalidade Geral". Nas opções de filtro, foram então selecionados, por ano, os termos "óbitos" e "asma" (código J45 na CID-10). Os critérios para as análises de regiões e estados seguiram os padrões da análise geral, com regiões e estados selecionados apenas em relação ao ano de 2010. As variáveis foram corrigidas pelas populações em 2010, de acordo com o censo do IBGE daquele ano.
Os resultados relativos à mortalidade por asma de pacientes hospitalizados referem-se ao total de óbitos por asma de pacientes hospitalizados, dividido pelo total de hospitalizações por asma e multiplicado por 100. No tocante às regiões e estados, para calcular o número de internações hospitalares por asma e de óbitos por asma em pacientes hospitalizados por 100.000 habitantes, as duas variáveis foram divididas pela população total do respectivo local e multiplicadas por 100.000, sendo usados apenas os dados de 2010. Todos os custos das hospitalizações por asma em reais (R$) foram convertidos em dólares norte-americanos (USD) com base na taxa de câmbio em 29/06/2016 (1,00 USD = R$ 3,237).
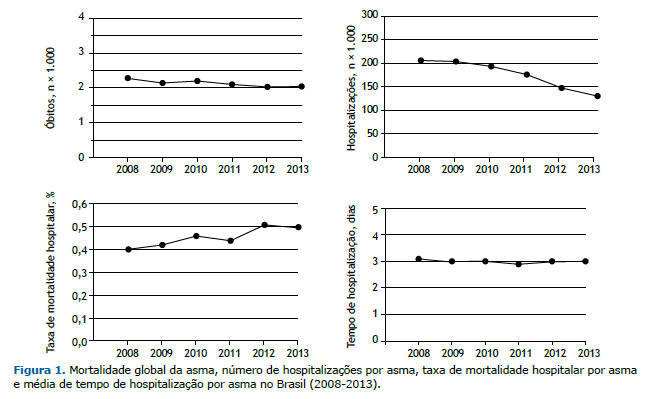
RESULTADOSO total de óbitos e hospitalizações por asma diminuiu de 2008 para 2013, não obstante os elevados números absolutos observados. Em 2013, último ano analisado, 2.047 pessoas morreram de asma no Brasil, isto é, aproximadamente 5 óbitos/dia e mais de 120.000 hospitalizações por ano. Em seis anos, houve redução de 10% e 36% do número absoluto de óbitos e hospitalizações por asma, respectivamente. No entanto, a taxa de mortalidade da asma em pacientes hospitalizados aumentou aproximadamente 25% durante esse período. A média de tempo de hospitalização por asma manteve-se em torno de 3 dias. Esses resultados são apresentados na Figura 1.
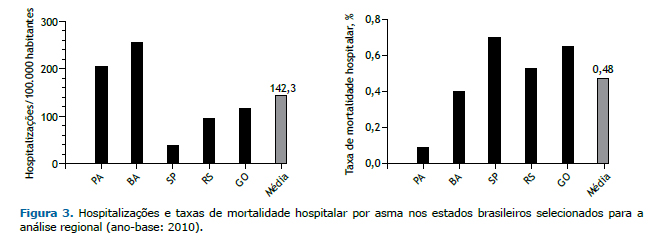
Geograficamente, analisamos o número de hospitalizações por asma e óbitos por asma em pacientes hospitalizados em 2010 por regiões e estados representativos. Ao analisarmos as diferentes regiões do Brasil, constatamos que as regiões Norte/Nordeste e Sudeste apresentaram as maiores taxas de hospitalizações por asma e óbitos por asma em pacientes hospitalizados, respectivamente. A média de hospitalizações por asma por região em 2010 foi de 110 hospitalizações/100.000 habitantes, e a proporção de óbitos entre pacientes hospitalizados foi de 0,46% (Figura 2). A média de tempo de hospitalização foi semelhante nas regiões, variando de 2,8 a 3,3 dias. Quando avaliamos os estados selecionados para representar as regiões do Brasil (Figura 3), observamos que os estados do Pará (região Norte) e Bahia (região Nordeste) apresentaram o maior número de hospitalizações por asma/100.000 habitantes. Os estados de São Paulo (região Sudeste), Goiás (região Centro-Oeste) e Rio Grande do Sul (região Sul) apresentaram números acima da média de óbitos por asma em pacientes hospitalizados. Em algumas regiões ou estados, houve discrepância entre o número de hospitalizações por asma/100.000 habitantes e a taxa de mortalidade em pacientes hospitalizados. A Figura 2 mostra que as regiões Norte e Nordeste apresentaram números acima da média de hospitalizações por asma, ao passo que as taxas de mortalidade estiveram abaixo da média. Por outro lado, a região Sudeste apresentou menos hospitalizações por asma, porém mais óbitos entre pacientes hospitalizados do que a média global. Além disso, a Figura 3 mostra a mesma discrepância nos estados do Pará e Bahia (mais hospitalizações por asma per capita e menos óbitos em pacientes hospitalizados), o oposto do que ocorreu no estado de São Paulo (menos hospitalizações por asma per capita e mais óbitos em pacientes hospitalizados).

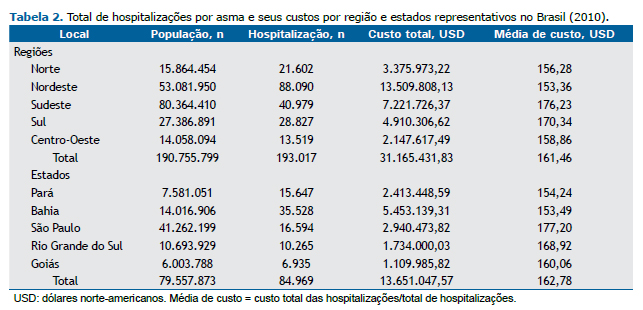
Finalmente, os custos das internações hospitalares por asma no Brasil diminuíram durante o período estudado, apesar da inflação econômica (Tabela 1). No entanto, o custo das hospitalizações ao sistema público de saúde chegou a quase 170 milhões de USD. A média de custo de cada hospitalização por asma foi de 160,00 USD (valores indexados e calculados pelo sistema público de saúde brasileiro). Além disso, a média de custo das hospitalizações por asma foi semelhante nas regiões e estados do Brasil (Tabela 2).

 DISCUSSÃO
DISCUSSÃOA asma, entre outras doenças respiratórias crônicas, é um importante problema mundial de saúde e tem impacto social negativo em diversas populações.(18) Infelizmente, para os governos de muitos países, a asma não é uma prioridade de saúde.(4) O Brasil tem alta prevalência de asma e asma grave, assim como outros países da América Latina.(6-8,13) No entanto, há poucos dados nacionais oficiais sobre o impacto da asma na América Latina. Nossos resultados mostram números longitudinais oficiais de óbitos e internações hospitalares por asma no maior país da América Latina, o que pode ajudar a melhorar o tratamento da asma em todo o país, a qualidade de vida dos pacientes e o controle dos custos da doença.
A mortalidade da asma no Brasil ainda é alta. Embora tenha havido uma pequena redução (de 10%) do total de óbitos de 2008 para 2013, aproximadamente 5 pacientes morrem de asma diariamente no Brasil. A mortalidade da asma infantil no Brasil também diminuiu de 1980 para 2000,(19) o que sugere uma tendência nacional de melhora lenta e gradual das taxas de óbito por asma no país. Em 2000, a maioria dos óbitos por asma ocorreu em hospitais, e os óbitos domiciliares foram mais comuns em pacientes idosos.(20) Além disso, uma análise prévia da mortalidade da asma no Brasil de 1998 a 2009 mostrou aumento da mortalidade em regiões menos desenvolvidas em comparação com regiões mais desenvolvidas. (21) Nos EUA, um dos países mais desenvolvidos do mundo, com mais de 300 milhões de habitantes, foram relatados 3.630 óbitos por asma em 2013 (aproximadamente 9,9 óbitos/dia). (22) Se considerarmos a população dos EUA e do Brasil nesse mesmo ano, as taxas de mortalidade da asma na população geral foram semelhantes em ambos os países, com aproximadamente 1 óbito/10.000 habitantes. Como a asma é uma doença tratável, óbitos por asma, muitas vezes prematuramente, deveriam ser uma fatalidade muito rara nesse contexto. As autoridades públicas, independentemente do grau de desenvolvimento do país, deveriam buscar continuamente a redução da mortalidade da asma.
As internações hospitalares em virtude de doenças respiratórias são um desfecho negativo na qualidade de vida dos pacientes e no sistema público de saúde. O DATASUS mostrou que o Brasil tem mais de 120.000 hospitalizações por asma por ano. No entanto, houve uma redução de 36% das internações hospitalares por asma durante o período analisado. Trata-se de um achado positivo para o sistema público de saúde do ponto de vista epidemiológico, e é difícil explicá-lo no contexto da análise do presente estudo. Uma possível explicação seria a implantação de uma política nacional de saúde pública pelo Ministério da Saúde em 2009, pela qual medicamentos para asma (beclometasona e salbutamol) passaram a ser fornecidos de maneira fácil e gratuita em todo o território do país.(23) É possível que essa política de saúde pública tenha facilitado o acesso a medicamentos de controle e resgate para pacientes com asma em todo o país. Nos EUA, as hospitalizações por asma permaneceram estáveis entre 2001 e 2009, com altos custos econômicos,(24,25) o que reforça a importância de uma revisão permanente dos programas de controle da asma pelos sistemas de saúde. No presente estudo, a mortalidade da asma em pacientes hospitalizados foi de aproximadamente 0,5%, com aumento de 25% durante o período de estudo. Assim, menos de 1% dos pacientes hospitalizados morrem de asma no Brasil. Esse achado sugere que o tratamento da asma grave em pacientes internados é aparentemente eficaz, o que indica que é imperativo realizar estudos abrangentes sobre os motivos pelos quais as taxas de óbito domiciliar por asma são tão altas no Brasil. Outro achado positivo foi o tempo de hospitalização por asma no Brasil. A média de tempo de hospitalização foi de 3 dias, independentemente de fatores geográficos, semelhante à de países desenvolvidos, tais como o Reino Unido.(26) Acreditamos que pouco possa ser modificado quanto às terapias convencionais disponíveis para pacientes internados em virtude dessa situação clínica grave, a fim de reduzir o número de dias de hospitalização.
A análise das regiões do Brasil mostrou que as regiões Norte/Nordeste (populações menos abastadas) e Sudeste (população mais abastada) apresentaram as maiores taxas de hospitalizações por asma e de óbitos por asma em pacientes hospitalizados, respectivamente. Os estados do Pará (região Norte) e Bahia (região Nordeste) apresentaram o maior número de hospitalizações por asma por 100.000 habitantes. Os estados de São Paulo (região Sudeste), Goiás (região Centro-Oeste) e Rio Grande do Sul (região Sul) apresentaram taxa acima da média de óbitos por asma em pacientes hospitalizados. Essas informações são importantes para as autoridades brasileiras de saúde pública e demandam análises mais minuciosas para melhorar o tratamento de pacientes com asma e os custos da doença. Nesse contexto, duas cidades brasileiras implantaram programas distintos de saúde pública para a asma (com a criação de centros de referência, facilidade de fornecimento de medicamentos, protocolos rigorosos de saúde pública e treinamento profissional) e conseguiram alcançar uma importante redução do número de hospitalizações por asma.(27,28) Além disso, em uma dessas cidades (Salvador, BA), o programa de controle da asma implantado mostrou que, quando pacientes com asma grave controlaram a doença, houve grande redução dos custos diretos da asma nas famílias (−89%) e aumento da renda familiar geral.(29) Essas iniciativas locais demonstram a importância da implantação de mais programas eficazes de controle da asma nos sistemas públicos de saúde.
Um achado interessante foi a discrepância entre o número de internações hospitalares por asma e as taxas de mortalidade da asma em pacientes hospitalizados nas diferentes regiões geográficas. As regiões Norte/Nordeste apresentaram hospitalizações por asma acima da média e mortalidade da asma abaixo da média. Por outro lado, a região Sudeste apresentou menos hospitalizações por asma e óbitos por asma em pacientes hospitalizados acima da média global. A mesma relação foi encontrada nos estados representativos selecionados no presente estudo (isto é, Pará/Bahia e São Paulo). Novamente, esses dados merecem uma análise minuciosa dos programas de controle da asma, levando-se em conta as diferenças regionais que são geralmente encontradas principalmente em países grandes.
A assistência hospitalar é o maior componente individual de custos diretos da asma na saúde pública. (30) Os custos das hospitalizações por asma em nossa análise acompanharam a redução do número de internações hospitalares, sem diferenças regionais, especialmente considerando a inflação econômica anual do período, que variou de 4,4% a 6,5%.(31) No entanto, mesmo com a redução das internações hospitalares por asma, o custo total das hospitalizações ainda foi alto. Quase 170 milhões de USD foram gastos com internações hospitalares por asma entre 2008 e 2013. A média de custo de uma hospitalização no Brasil é de aproximadamente 160,00 USD. Pode-se considerar que o custo de uma hospitalização no Brasil é baixo, mas é importante notar que se trata de um valor calculado pelo governo, pago aos serviços públicos de saúde (hospitais), e que, na verdade, não reflete o montante real gasto pelos próprios hospitais. A questão do custo da doença estipulado pelo governo brasileiro (informado pelo DATASUS) e o custo "real" para o serviço de saúde é outro aspecto que merece ampla análise e discussão pública, além de uma revisão administrativa e financeira. Uma revisão sistemática recente dos custos da asma grave no Brasil mostrou que as principais despesas diretas estavam relacionadas com hospitalizações e medicamentos e que foram gastos 733,00 USD por paciente por ano, o que ressalta os elevados custos econômicos da asma.(32)
Nosso estudo tem limitações. Trata-se de uma análise retrospectiva de dados secundários, que estão sujeitos à incompletude dos prontuários médicos, inclusive diagnóstico errôneo da doença. O subdiagnóstico e a subnotificação são problemas em qualquer sistema de saúde, particularmente em países em desenvolvimento. (33) No entanto, é preciso considerar que os dados coletados representam os números oficiais do governo brasileiro, e limitações podem ser encontradas em qualquer país que implante esse tipo de banco de dados. Não obstante, acreditamos que o DATASUS, com todas as suas limitações, ajuda substancialmente a apresentar informações relevantes sobre o impacto da asma no Brasil.
Em suma, a mortalidade da asma no Brasil ainda é muito alta se levarmos em conta que a asma é uma doença tratável. Apesar da diminuição das hospitalizações por asma nos últimos anos, os números absolutos ainda são notáveis e resultam em relevantes custos diretos e indiretos à sociedade. Finalmente, esses resultados mostram que a asma deveria receber mais atenção das autoridades de saúde pública do Brasil e da maioria dos outros países da América Latina.
REFERÊNCIAS1. Eder W, Ege MJ, von Mutius E. The asthma epidemic. N Engl J Med. 2006;355(21):2226-35. https://doi.org/10.1056/NEJMra054308
2. Global Initiative for Asthma [homepage on the Internet]. Bethesda: Global Initiative for Asthma [cited 2016 Jun 07]. Global Strategy for Asthma Management and Prevention 2016. [Adobe Acrobat document, 151p.]. Available from: http://ginasthma.org/wp-content/uploads/2016/04/wms-GINA-2016-main-report-final.pdf
3. Terzano C, Cremonesi G, Girbino G, Ingrassia E, Marsico S, Nicolini G, et al. 1-year prospective real life monitoring of asthma control and quality of life in Italy. Respir Res. 2012;13:112. https://doi.org/10.1186/1465-9921-13-112
4. Braman SS. The global burden of asthma. Chest. 2006;130(1 Suppl):4S-12S. https://doi.org/10.1378/chest.130.1_suppl.4S
5. Pitrez PM, Stein RT. Asthma in Latin America: the dawn of a new epidemic. Curr Opin Allergy Clin Immunol. 2008;8(5):378-83. https://doi.org/10.1097/ACI.0b013e32830fb911
6. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. The International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Lancet. 1998;351(9111):1225-32. https://doi.org/10.1016/S0140-6736(97)07302-9
7. Lai CK, Beasley R, Crane J, Foliaki S, Shah J, Weiland S; et al. Global variation in the prevalence and severity of asthma symptoms: phase three of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax. 2009;64(6):476-83. https://doi.org/10.1136/thx.2008.106609
8. Chong Neto HJ, Rosário NA, Solé D ; Latin American ISAAC Group. Asthma and Rhinitis in South America: How Different They are From Other Parts of the World. Allergy Asthma Immunol Res. 2012;4(2):62-7. https://doi.org/10.4168/aair.2012.4.2.62
9. Solé D, Rosário Filho NA, Sarinho ES, Camelo-Nunes IC, Barreto BA, Medeiros ML, et al. Prevalence of asthma and allergic diseases in adolescents: nine-year follow-up study (2003-2012). J Pediatr (Rio J). 2015;91(1):30-5. https://doi.org/10.1016/j.jped.2014.05.002
10. Kuschnir FC, Gurgel RQ, Solé D, Costa E, Felix MM, de Oliveira CL, et al. ERICA: prevalence of asthma in Brazilian adolescents. Rev Saude Publica. 2016;50 Suppl 1:13s. https://doi.org/10.1590/s01518-8787.2016050006682
11. Mancilla-Hernández EM, González-Solórzano EV, Medina-Ávalos MÁ, Barnica-Alvarado RH. Prevalence of asthma and its symptoms in schoolchildren from Cuernavaca, Morelos, Mexico [Article in Spanish]. Rev Alerg Mex. 2016;63(4):351-7.
12. Mallol J, Crane J, von Mutius E, Odhiambo J, Keil U, Stewart A; et al. The International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three: a global synthesis. Allergol Immunopathol (Madr). 2013;41(2):73-85. https://doi.org/10.1016/j.aller.2012.03.001
13. Mallol J, Solé D, Baeza-Bacab M, Aguirre-Camposano V, Soto-Quiros M, Baena-Cagnani C, et al. Regional variation in asthma symptom prevalence in Latin American children. J Asthma. 2010;47(6):644-50. https://doi.org/10.3109/02770901003686480
14. Simões SM, Cunha SS, Barreto ML, Cruz AA. Distribution of severity of asthma in childhood. J Pediatr (Rio J). 2010;86(5):417-23. https://doi.org/10.1590/S0021-75572010000500011
15. Roncada C, de Oliveira SG, Cidade SF, Sarria EE, Mattiello R, Ojeda BS, et al. Burden of asthma among inner-city children from Southern Brazil. J Asthma. 2016;53(5):498-504. https://doi.org/10.3109/02770903.2015.1108438
16. Brasil. Departamento de Informática do Sistema Único de Saúde--DATASUS [homepage on the Internet]. Brasília: DATASUS [cited 2016 Jun 07]. Available from: http://datasus.saude.gov.br/informacoes-de-saude/tabnet
17. Instituto Brasileiro de Geografia e Estatística [homepage on the Internet]. São Paulo: IBGE [cited 2016 Jun 20]. Informações de Saúde (TABNET) Available from: http://www.ibge.gov.br/home/
18. Bousquet J, Bousquet PJ, Godard P, Daures JP. The public health implications of asthma. Bull World Health Organ. 2005;83(7):548-54.
19. Prietsch SO, Zhang L, Catharino AR, Vauchinski L, Rodrigues FE. Asthma mortality among Brazilian children up to 19 years old between 1980 and 2007. J Pediatr (Rio J). 2012;88(5):384-8. https://doi.org/10.2223/jped.2215
20. Santo AH. Asthma-related mortality, Brazil, 2000: a study using multiple causes of death [Article in Portuguese]. Cad Saude Publica. 2006;22(1):41-52. https://doi.org/10.1590/S0102-311X2006000100005
21. de Souza-Machado C, Souza-Machado A, Cruz AA. Asthma mortality inequalities in Brazil: tolerating the unbearable. ScientificWorldJournal. 2012;2012:625829. https://doi.org/10.1100/2012/625829
22. Centers for Disease Control and Prevention [homepage on the Internet].Atlanta: CDC [cited 2016 Jul 20]. National Center of Health Statistics--Asthma. Available from: http://www.cdc.gov/nchs/fastats/asthma.htm
23. Brasil. Ministério da Saúde. Portal da Saúde [homepage on the Internet]. Brasília: Ministério da Saúde [cited 2016 Jul 20]. Programa Farmácia Popular do Brasil. Available from: http://portalsaude.saude.gov.br/index.php/o-ministerio/principal/secretarias/sctie/farmacia-popular
24. Moorman JE, Akinbami LJ, Bailey CM, Zahran HS, King ME, Johnson CA, et al. National surveillance of asthma: United States, 2001-2010. Vital Health Stat 3. 2012;(35):1-58.
25. Sullivan PW, Ghushchyan VH, Slejko JF, Belozeroff V, Globe DR, Lin SL. The burden of adult asthma in the United States: evidence from the Medical Expenditure Panel Survey. J Allergy Clin Immunol. 2011;127(2):363-369.e1-3.
26. Soyiri IN, Reidpath DD, Sarran C. Asthma length of stay in hospitals in London 2001-2006: demographic, diagnostic and temporal factors. PLoS One. 2011;6(11):e27184. https://doi.org/10.1371/journal.pone.0027184
27. Ponte EV, Petroni J, Ramos DC, Pimentel L, Freitas DN, Cruz AA. Perception of asthma control in asthma patients. J Bras Pneumol. 2007;33(6):635-40. https://doi.org/10.1590/S1806-37132007000600005
28. Cerci Neto A, Ferreira Filho OF, Bueno T, Talhari MA. Reduction in the number of asthma-related hospital admissions after the implementation of a multidisciplinary asthma control program in the city of Londrina, Brazil. J Bras Pneumol. 2008;34(9):639-45.
29. Franco R, Nascimento HF, Cruz AA, Santos AC, Souza-Machado C, Ponte EV, et al. The economic impact of severe asthma to low-income families. Allergy. 2009;64(3):478-83. https://doi.org/10.1111/j.1398-9995.2009.01981.x
30. Bahadori K, Doyle-Waters MM, Marra C, Lynd L, Alasaly K, Swiston J, et al. Economic burden of asthma: a systematic review. BMC Pulm Med. 2009;9:24. https://doi.org/10.1186/1471-2466-9-24
31. Global-Rates.com [homepage on the Internet]. Utrecht, Netherlands: Triami Media BV. Inflação Brasil - índice de preços ao consumidor (IPC) [cited 2016 Jul 20]. Available from: http://pt.global-rates.com/estatisticas-economicas/inflacao/indice-de-precos-ao-consumidor/ipc/brasil.aspx
32. Stirbulov R, Lopes da Silva N, Maia SC, Carvalho-Netto E, Angelini L. Cost of severe asthma in Brazil-systematic review. J Asthma. 2016;53(10):1063-70. https://doi.org/10.3109/02770903.2016.1171338
33. Martins P, Rosado-Pinto J, do Ceu Teixeira M, Neuparth N, Silva O, Tavares H, et al. Under-report and underdiagnosis of chronic respiratory diseases in an African country. Allergy. 2009;64(7):1061-7. https://doi.org/10.1111/j.1398-9995.2009.01956.x












 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket