ABSTRACT
Objective: To present official longitudinal data on the impact of asthma in Brazil between 2008 and 2013. Methods: This was a descriptive study of data collected between 2008 and 2013 from an official Brazilian national database, including data on asthma-related number of hospitalizations, mortality, and hospitalization costs. A geographical subanalysis was also performed. Results: In 2013, 2,047 people died from asthma in Brazil (5 deaths/day), with more than 120,000 asthma-related hospitalizations. During the whole study period, the absolute number of asthma-related deaths and of hospitalizations decreased by 10% and 36%, respectively. However, the in-hospital mortality rate increased by approximately 25% in that period. The geographic subanalysis showed that the northern/northeastern and southeastern regions had the highest asthma-related hospitalization and in-hospital mortality rates, respectively. An analysis of the states representative of the regions of Brazil revealed discrepancies between the numbers of asthma-related hospitalizations and asthma-related in-hospital mortality rates. During the study period, the cost of asthma-related hospitalizations to the public health care system was US$ 170 million. Conclusions: Although the numbers of asthma-related deaths and hospital admissions in Brazil have been decreasing since 2009, the absolute numbers are still high, resulting in elevated direct and indirect costs for the society. This shows the relevance of the burden of asthma in middle-income countries.
Keywords:
Asthma/epidemiology; Asthma/mortality; Public health; Hospitalization.
RESUMO
Objetivo: Apresentar dados longitudinais oficiais sobre o impacto da asma no Brasil entre 2008 e 2013. Métodos: Estudo descritivo de dados extraídos de um banco de dados do governo brasileiro entre 2008 e 2013, no qual foram analisados as hospitalizações e óbitos por asma, bem como o custo das hospitalizações. Foi também realizada uma subanálise geográfica. Resultados: Em 2013, 2.047 pessoas morreram de asma no Brasil (5 óbitos/dia), com mais de 120.000 hospitalizações por asma. Durante o período de estudo, o número absoluto de óbitos e hospitalizações por asma diminuiu 10% e 36%, respectivamente. No entanto, a taxa de mortalidade hospitalar aumentou aproximadamente 25%. A subanálise geográfica mostrou que as regiões Norte/Nordeste e Sudeste apresentaram as maiores taxas de hospitalização e mortalidade hospitalar por asma, respectivamente. A análise dos estados representativos de cada região mostrou discrepâncias entre as hospitalizações por asma e as taxas de mortalidade hospitalar por asma. Durante o período de estudo, as hospitalizações por asma custaram US$ 170 milhões ao sistema público de saúde. Conclusões: Embora os óbitos e hospitalizações por asma no Brasil estejam diminuindo desde 2009, os números absolutos ainda são altos, com elevados custos diretos e indiretos para a sociedade, o que mostra a relevância do impacto da asma em países de renda média.
Palavras-chave:
Asma/epidemiologia; Asma/mortalidade; Saúde pública; Hospitalização.
INTRODUCTIONAsthma is a treatable chronic disease of the airways that affects all age groups and has high prevalence, morbidity, and mortality around the world.(1,2) Many patients live with uncontrolled asthma, causing impaired quality of life and resulting in direct and indirect costs for societies, particularly in developing countries.(3-5) The prevalence of asthma (including severe asthma) is high in various countries, with a relevant impact on global public health care.(6,7) The populations in which the prevalence of asthma is highest (> 20%) are observed in English-speaking countries and in Latin America.(8)
The prevalence of childhood asthma in Latin America varies widely (4-30% in children), but it is above 10% in virtually all countries.(9-12) The high burden of asthma in those countries is usually complicated by the limited access to health care and essential medications.(4,8,13) Brazil, a middle-income country of continental size, is one of the countries with the highest prevalences of asthma in children, with high rates of severe asthma.(6,7,14) We have recently shown that, in southern Brazil, 20% of school-age children have asthma, many of whom lacking control of the disease and presenting with high rates of physical inactivity, school absenteeism, and hospitalizations.(15) However, national data on the impact of asthma in developing countries are scarce. Data on mortality and number of hospitalizations regarding a particular disease are important to guide public health care policies. Large national databases are uncommon in developing countries. However, when available, such data become valuable information for improving health care policies for prevalent diseases.
Brazil has an official and longitudinal free-access database from the Brazilian Unified Health Care System, which records health indicators, such as mortality rates and number/costs of hospitalizations.(16) Thus, the aim of our study was to present longitudinal data regarding the impact of asthma in Brazil in recent years and to analyze geographic factors concerning the disease.
METHODSWe conducted a descriptive study, based on asthma information collected from the Departamento de Informática do Sistema Único de Saúde (DATASUS, Information Technology Department of the Brazilian Unified Health Care System) database.(16) The population studied consisted of all cases of asthma -in accordance with the International Classification of Diseases, 10th revision (ICD-10; code J.45)-in which hospitalizations and deaths were reported between 2008 and 2013. For the geographic analysis, variables were corrected for population numbers in 2010, according to regions and states, using another database: the Instituto Brasileiro de Geografia e Estatística (IBGE, Brazilian Institute of Geography and Statistics) database, which provides data regarding the Brazilian population via periodic censuses.(17) Graphics were prepared using the GraphPad Prism statistical software program, version 6 (GraphPad Inc., San Diego, CA, USA). The DATASUS database is under public domain; hence, approval of our research ethics committee was not required.
Data from the DATASUS database were subdivided into three groups for analysis: Brazil, regions, and states. The following variables were analyzed: number of deaths, number of hospitalizations, length of hospital stay, and financial costs of hospitalization.
For the general analysis, our survey was carried out from 2008 to 2013, using the Health Information System tool. For the variables analyzed, we used the tables of Epidemiology and Morbidity in the "Hospital Morbidity" group, and then the "General, by hospital location" sub-item. In the filter options, the items "years", "contents of hospitalizations", "mean length of hospital stay", "total cost", "mean cost of hospitalization", and "deaths" were selected and correlated with "asthma" (ICD-10 code, J.45). Data regarding total deaths, aiming to cover all cases of asthma-related deaths and not only those related to hospitalizations, were collected from the Brazilian National Mortality Database, using the "Vital Statistics" item (Mortality Group, 1996 to 2014) and the "General Mortality" sub-item. In the filter options, we then selected, per year, the terms "deaths" and "asthma" (ICD-10, code J.45). The criteria for the analyses of regions and states followed the standards of the general analysis, with regions and states selected only regarding the year of 2010. The variables were corrected by the populations in 2010, in accordance with the IBGE census of that year.
The results concerning asthma-related mortality of hospitalized patients refer to the total number of asthma-related deaths of hospitalized patients, divided by the total number of hospitalizations due to asthma, and multiplied by 100. In relation to the regions and states, in order to calculate the numbers of asthma-related hospital admissions and asthma-related deaths of hospitalized patients per 100,000 population, both variables were divided by the total population of the respective location and multiplied by 100,000, using only the data from 2010. All asthma-related costs of hospitalizations in Brazilian reals (R$) were converted to American dollars (USD), on the basis of the exchange rate on June 29, 2016 (USD 1.00 = R$ 3,237).
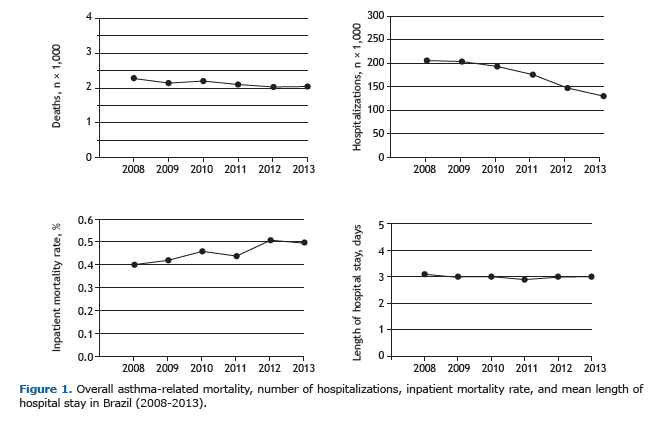
RESULTSThe total numbers of asthma-related total deaths and of hospitalizations decreased from 2008 to 2013, despite the high absolute numbers observed. In 2013, the last year analyzed, 2,047 people died from asthma in Brazil, meaning approximately 5 deaths/day and more than 120,000 hospitalizations per year. In six years, the absolute numbers of asthma-related deaths and hospitalizations decreased by 10% and 36%, respectively. However, the asthma-related mortality rate in hospitalized patients increased by approximately 25% during that period. The mean length of hospital stay due to asthma remained at approximately 3 days. These results are presented in Figure 1.
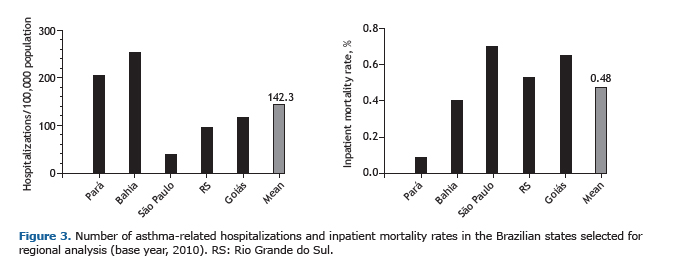
Geographically, we analyzed the numbers of asthma-related hospitalizations and deaths in hospitalized patients in 2010 by regions and representative states. Analyzing the different regions of Brazil, we found that the northern/northeastern and southeastern regions showed the highest rates of asthma-related hospitalizations and deaths of hospitalized patients, respectively. The mean number of asthma-related hospitalizations by region in 2010 was 110 hospitalizations/100,000 population, and the proportion of deaths among hospitalized patients was 0.46% (Figure 2). The mean length of hospital stay was similar among the regions, ranging from 2.8 to 3.3 days. When we evaluated the states selected to represent the regions of Brazil (Figure 3), we observed that the states of Pará (northern region) and Bahia (northeastern region) had the largest numbers of asthma-related hospitalizations/100,000 population. The states of São Paulo (southeastern region), Goiás (central-west region), and Rio Grande do Sul (southern region) revealed numbers of asthma-related deaths among hospitalized patients above the mean. We also observed that, in some regions or states, there was a discrepancy between the number of asthma-related hospitalizations/100,000 population and the mortality rate in hospitalized patients. Figure 2 shows that the northern and northeastern regions had numbers of asthma-related hospitalizations above the mean, whereas the mortality rates were below the mean. In contrast, the southeastern region had fewer asthma-related hospitalizations but more deaths among hospitalized patients than the overall mean. In addition, Figure 3 shows the same discrepancy in the states of Pará and Bahia (more asthma-related hospitalizations per capita and fewer deaths in hospitalized patients), which was the opposite in the state of São Paulo (fewer asthma-related hospitalizations per capita and more deaths in hospitalized patients).

Finally, the asthma-related costs of hospital admissions in Brazil decreased during the period studied, despite the economic inflation (Table 1). However, the cost of hospitalizations to the public health care system reached almost USD 170 million. The mean cost of each asthma-related hospitalization was USD 160.00 (values indexed and calculated by the Brazilian public health care system). In addition, the mean cost of asthma-related hospitalizations was similar among the regions and the states of Brazil (Table 2).

 DISCUSSION
DISCUSSIONAsthma, among other chronic respiratory diseases, represents an important global health problem, resulting in a negative social impact on various populations.(18) Unfortunately, for the governments of many countries, asthma is not a health care priority.(4) Brazil has a high prevalence of asthma and severe asthma, which is also observed in other countries in Latin America.(6-8,13) Nevertheless, there is a lack of official national data on the impact of asthma in Latin America. Our results show official longitudinal numbers of asthma-related deaths and hospital admissions in the largest country of Latin America, which might help to improve national asthma care, the quality of life of patients, and the control of costs of the disease.
Asthma-related mortality in Brazil is still high. Although we observed a small reduction (10%) in the total number of deaths from 2008 to 2013, approximately 5 patients die from asthma daily in Brazil. Childhood asthma-related mortality in Brazil also decreased from 1980 to 2000,(19) suggesting a national trend toward a slow and gradual improvement in asthma-related deaths in the country. In 2000, most asthma-related deaths occurred in hospitals, and household deaths were more common in elderly patients.(20) In addition, one previous analysis of asthma-related mortality in Brazil from 1998 to 2009 showed increased mortality in less developed regions in comparison with more developed regions.(21) In the USA, one of the most developed countries in the world, with a population of over 300 million inhabitants, 3,630 deaths due to asthma were reported in 2013 (approximately 9.9 deaths/day).(22) Considering the population in the USA and in Brazil in that particular year, the asthma-related mortality rates were similar in the general population in both countries, with approximately 1 death/10,000 population. Given that asthma is a treatable disease, deaths due to asthma, often prematurely, should be a very rare fatality in this context. Public authorities, regardless of the degree of development of the country, should be continuously pursuing a reduction in asthma-related mortality.
Hospital admissions due to respiratory diseases are a negative outcome in the quality of life of patients and in the public health care system. DATASUS showed that Brazil has more than 120,000 asthma-related hospitalizations per year. However, there was a reduction of 36% of asthma-related hospital admissions during the period analyzed. This is a positive finding for the public health care system from an epidemiological point of view, and it is difficult to explain it in the context of the analysis of the present study. One possible explanation could be the implementation of a national public health care policy by the Brazilian National Ministry of Health, implemented in 2009, which provided free and easily accessible asthma medications (beclomethasone and albuterol) in the whole territory of the country.(23) This public health care policy might have facilitated the access to control and rescue medications for asthma patients across the country. In the USA, hospitalizations due to asthma remained stable between 2001 and 2009, with high economic costs,(24,25) emphasizing the importance of a permanent review of asthma control programs by health care systems. In the present study, we showed that asthma-related mortality in hospitalized patients was around 0.5%, with a 25% increase during the study period. Hence, less than 1% of hospitalized patients die from asthma in Brazil. This finding suggests that the management of severe asthma in inpatients appears to be effective, indicating that it is imperative that comprehensive studies on the reasons why household asthma-related deaths are so high in Brazil be conducted. Another positive finding was the length of asthma-related hospital stay in Brazil. The mean length of hospital stay was 3 days, regardless of geographic factors, which is similar to that in developed countries, such as the United Kingdom.(26) We believe that little can be modified regarding the inpatient conventional therapies available against this severe clinical situation in order to reduce the number of hospital days.
When the regions of Brazil were analyzed, the northern\northeastern regions (less affluent populations) and the southeastern region (the most affluent population) showed the highest rates of asthma-related hospitalizations and deaths of hospitalized patients, respectively. The states of Pará (northern region) and Bahia (northeastern region) had the largest numbers of asthma-related hospitalizations per 100,000 population. The states of São Paulo (southeastern region), Goiás (central-west region), and Rio Grande do Sul (southern region) had a rate of asthma-related deaths among hospitalized patients above the mean. This information is important for the Brazilian public health care authorities and requires more detailed analyses in order to improve the management of asthma patients and asthma-related costs. In this context, two Brazilian cities implemented distinct public health care programs for asthma (with the creation of referral centers, easy provision of medications, strict public health care protocols, and professional training) and were successful in achieving an important decrease in the number of asthma-related hospitalizations.(27,28) Moreover, in one of these cities (Salvador, in the state of Bahia), the implemented asthma control program showed that, when patients with severe asthma had their disease under control, there was a major decrease in the direct costs of asthma in the families (−89%) and an increase in the overall family income.(29) These local initiatives demonstrate the importance of implementing further effective asthma control programs in public health care systems.
An interesting finding was the discrepancy between the number of asthma-related hospital admissions and asthma-related mortality rates in hospitalized patients among the geographic regions. The northern\northeastern regions showed asthma-related hospitalizations above the mean, which was the opposite regarding asthma-related mortality. In contrast, the southeastern region had fewer asthma-related hospitalizations but more asthma-related deaths in hospitalized patients than the overall mean. The same relationship was found in the representative states selected in the present study (i.e., Pará/Bahia and São Paulo). Once again, these data deserve an in-depth analysis by asthma control programs, considering the regional differences that are usually found particularly in large countries.
Inpatient care is the largest single component of direct asthma-related costs in public health.(30) The costs of asthma-related hospitalizations in our analysis followed the reduction in the number of hospital admissions observed, with no regional differences, especially considering the annual economic inflation of the period, which ranged from 4.4% to 6.5%.(31) Nevertheless, even with the reduction in asthma-related hospital admissions, the total cost of hospitalizations was still high. Almost USD 170 million were spent on asthma-related hospital admissions between 2008 and 2013. The mean cost of one hospitalization in Brazil is approximately USD 160.00. One may consider that the cost of one hospitalization in Brazil is low, but it is important to note that this is a value calculated by the government, which is paid to public health care providers (hospitals), and that, in fact, does not reflect the actual amount spent by the hospitals themselves. The issue of the cost of the disease stipulated by the Brazilian government (informed by DATASUS) and the "real" cost for the health care provider is another aspect that deserves public comprehensive public analysis and discussion, as well as an administrative-financial review. A recent systematic review of the costs of severe asthma in Brazil showed that the major direct expenses were related to hospitalizations and medications and that USD 733.00 were spent per patient per year, highlighting the elevated economic costs of asthma.(32)
Our study has limitations. This was a retrospective analysis of secondary data, which are subject to inadequate completion of medical records, including erroneous diagnosis of the disease. Underdiagnosis and underreporting are problems in any health care system, particularly in developing countries.(33) However, we have to consider that the data collected represent the official numbers of the Brazilian government, and limitations can be found in any country that implements this type of database. Nevertheless, we believe that DATASUS, with all its limitations, substantially helps to present relevant information on the impact of asthma in Brazil.
In conclusion, asthma-related mortality in Brazil is still very high if we take into account that asthma is a treatable disease. Despite the decrease in the number of asthma-related hospitalizations in recent years, the absolute numbers are still remarkable, resulting in relevant direct and indirect costs for the society. Finally, these results show that asthma should receive greater attention from the public health care authorities in Brazil and most other countries in Latin America.
REFERENCES1. Eder W, Ege MJ, von Mutius E. The asthma epidemic. N Engl J Med. 2006;355(21):2226-35. https://doi.org/10.1056/NEJMra054308
2. Global Initiative for Asthma [homepage on the Internet]. Bethesda: Global Initiative for Asthma [cited 2016 Jun 07]. Global Strategy for Asthma Management and Prevention 2016. [Adobe Acrobat document, 151p.]. Available from: http://ginasthma.org/wp-content/uploads/2016/04/wms-GINA-2016-main-report-final.pdf
3. Terzano C, Cremonesi G, Girbino G, Ingrassia E, Marsico S, Nicolini G, et al. 1-year prospective real life monitoring of asthma control and quality of life in Italy. Respir Res. 2012;13:112. https://doi.org/10.1186/1465-9921-13-112
4. Braman SS. The global burden of asthma. Chest. 2006;130(1 Suppl):4S-12S. https://doi.org/10.1378/chest.130.1_suppl.4S
5. Pitrez PM, Stein RT. Asthma in Latin America: the dawn of a new epidemic. Curr Opin Allergy Clin Immunol. 2008;8(5):378-83. https://doi.org/10.1097/ACI.0b013e32830fb911
6. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. The International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Lancet. 1998;351(9111):1225-32. https://doi.org/10.1016/S0140-6736(97)07302-9
7. Lai CK, Beasley R, Crane J, Foliaki S, Shah J, Weiland S; et al. Global variation in the prevalence and severity of asthma symptoms: phase three of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax. 2009;64(6):476-83. https://doi.org/10.1136/thx.2008.106609
8. Chong Neto HJ, Rosário NA, Solé D; Latin American ISAAC Group. Asthma and Rhinitis in South America: How Different They are From Other Parts of the World. Allergy Asthma Immunol Res. 2012;4(2):62-7. https://doi.org/10.4168/aair.2012.4.2.62
9. Solé D, Rosário Filho NA, Sarinho ES, Camelo-Nunes IC, Barreto BA, Medeiros ML, et al. Prevalence of asthma and allergic diseases in adolescents: nine-year follow-up study (2003-2012). J Pediatr (Rio J). 2015;91(1):30-5. https://doi.org/10.1016/j.jped.2014.05.002
10. Kuschnir FC, Gurgel RQ, Solé D, Costa E, Felix MM, de Oliveira CL, et al. ERICA: prevalence of asthma in Brazilian adolescents. Rev Saude Publica. 2016;50 Suppl 1:13s. https://doi.org/10.1590/s01518-8787.2016050006682
11. Mancilla-Hernández EM, González-Solórzano EV, Medina-Ávalos MÁ, Barnica-Alvarado RH. Prevalence of asthma and its symptoms in schoolchildren from Cuernavaca, Morelos, Mexico [Article in Spanish]. Rev Alerg Mex. 2016;63(4):351-7.
12. Mallol J, Crane J, von Mutius E, Odhiambo J, Keil U, Stewart A; et al. The International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three: a global synthesis. Allergol Immunopathol (Madr). 2013;41(2):73-85. https://doi.org/10.1016/j.aller.2012.03.001
13. Mallol J, Solé D, Baeza-Bacab M, Aguirre-Camposano V, Soto-Quiros M, Baena-Cagnani C, et al. Regional variation in asthma symptom prevalence in Latin American children. J Asthma. 2010;47(6):644-50. https://doi.org/10.3109/02770901003686480
14. Simões SM, Cunha SS, Barreto ML, Cruz AA. Distribution of severity of asthma in childhood. J Pediatr (Rio J). 2010;86(5):417-23. https://doi.org/10.1590/S0021-75572010000500011
15. Roncada C, de Oliveira SG, Cidade SF, Sarria EE, Mattiello R, Ojeda BS, et al. Burden of asthma among inner-city children from Southern Brazil. J Asthma. 2016;53(5):498-504. https://doi.org/10.3109/02770903.2015.1108438
16. Brasil. Departamento de Informática do Sistema Único de Saúde--DATASUS [homepage on the Internet]. Brasília: DATASUS [cited 2016 Jun 07]. Available from: http://datasus.saude.gov.br/informacoes-de-saude/tabnet
17. Instituto Brasileiro de Geografia e Estatística [homepage on the Internet]. São Paulo: IBGE [cited 2016 Jun 20]. Informações de Saúde (TABNET) Available from: http://www.ibge.gov.br/home/
18. Bousquet J, Bousquet PJ, Godard P, Daures JP. The public health implications of asthma. Bull World Health Organ. 2005;83(7):548-54.
19. Prietsch SO, Zhang L, Catharino AR, Vauchinski L, Rodrigues FE. Asthma mortality among Brazilian children up to 19 years old between 1980 and 2007. J Pediatr (Rio J). 2012;88(5):384-8. https://doi.org/10.2223/jped.2215
20. Santo AH. Asthma-related mortality, Brazil, 2000: a study using multiple causes of death [Article in Portuguese]. Cad Saude Publica. 2006;22(1):41-52. https://doi.org/10.1590/S0102-311X2006000100005
21. de Souza-Machado C, Souza-Machado A, Cruz AA. Asthma mortality inequalities in Brazil: tolerating the unbearable. ScientificWorldJournal. 2012;2012:625829. https://doi.org/10.1100/2012/625829
22. Centers for Disease Control and Prevention [homepage on the Internet].Atlanta: CDC [cited 2016 Jul 20]. National Center of Health Statistics--Asthma. Available from: http://www.cdc.gov/nchs/fastats/asthma.htm
23. Brasil. Ministério da Saúde. Portal da Saúde [homepage on the Internet]. Brasília: Ministério da Saúde [cited 2016 Jul 20]. Programa Farmácia Popular do Brasil. Available from: http://portalsaude.saude.gov.br/index.php/o-ministerio/principal/secretarias/sctie/farmacia-popular
24. Moorman JE, Akinbami LJ, Bailey CM, Zahran HS, King ME, Johnson CA, et al. National surveillance of asthma: United States, 2001-2010. Vital Health Stat 3. 2012;(35):1-58.
25. Sullivan PW, Ghushchyan VH, Slejko JF, Belozeroff V, Globe DR, Lin SL. The burden of adult asthma in the United States: evidence from the Medical Expenditure Panel Survey. J Allergy Clin Immunol. 2011;127(2):363-369.e1-3.
26. Soyiri IN, Reidpath DD, Sarran C. Asthma length of stay in hospitals in London 2001-2006: demographic, diagnostic and temporal factors. PLoS One. 2011;6(11):e27184. https://doi.org/10.1371/journal.pone.0027184
27. Ponte EV, Petroni J, Ramos DC, Pimentel L, Freitas DN, Cruz AA. Perception of asthma control in asthma patients. J Bras Pneumol. 2007;33(6):635-40. https://doi.org/10.1590/S1806-37132007000600005
28. Cerci Neto A, Ferreira Filho OF, Bueno T, Talhari MA. Reduction in the number of asthma-related hospital admissions after the implementation of a multidisciplinary asthma control program in the city of Londrina, Brazil. J Bras Pneumol. 2008;34(9):639-45.
29. Franco R, Nascimento HF, Cruz AA, Santos AC, Souza-Machado C, Ponte EV, et al. The economic impact of severe asthma to low-income families. Allergy. 2009;64(3):478-83. https://doi.org/10.1111/j.1398-9995.2009.01981.x
30. Bahadori K, Doyle-Waters MM, Marra C, Lynd L, Alasaly K, Swiston J, et al. Economic burden of asthma: a systematic review. BMC Pulm Med. 2009;9:24. https://doi.org/10.1186/1471-2466-9-24
31. Global-Rates.com [homepage on the Internet]. Utrecht, Netherlands: Triami Media BV. Inflação Brasil - índice de preços ao consumidor (IPC) [cited 2016 Jul 20]. Available from: http://pt.global-rates.com/estatisticas-economicas/inflacao/indice-de-precos-ao-consumidor/ipc/brasil.aspx
32. Stirbulov R, Lopes da Silva N, Maia SC, Carvalho-Netto E, Angelini L. Cost of severe asthma in Brazil-systematic review. J Asthma. 2016;53(10):1063-70. https://doi.org/10.3109/02770903.2016.1171338
33. Martins P, Rosado-Pinto J, do Ceu Teixeira M, Neuparth N, Silva O, Tavares H, et al. Under-report and underdiagnosis of chronic respiratory diseases in an African country. Allergy. 2009;64(7):1061-7. https://doi.org/10.1111/j.1398-9995.2009.01956.x











 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket