ABSTRACT
Pulmonary artery dissection is a fatal complication of long-standing pulmonary hypertension, manifesting as acute, stabbing chest pain, progressive dyspnea, cardiogenic shock, or sudden death. Its incidence has been underestimated, and therapeutic options are still scarce. In patients with pulmonary hypertension, new chest pain, acute chest pain, or cardiogenic shock should raise the suspicion of pulmonary artery dissection, which can result in sudden death.
Keywords:
Hypertension, pulmonary; Chest pain; Pulmonary artery.
RESUMO
A dissecção da artéria pulmonar é uma complicação fatal da hipertensão pulmonar de longa duração que se manifesta como dor torácica aguda e lancinante, dispneia progressiva, choque cardiogênico ou morte súbita. Sua incidência é subestimada, e as opções terapêuticas são ainda limitadas. O aparecimento de uma dor torácica aguda ou nova, choque cardiogênico ou morte súbita em pacientes portadores de hipertensão pulmonar deve alertar para o diagnóstico de dissecção da artéria pulmonar.
Palavras-chave:
Hipertensão pulmonar; Dor no peito; Artéria pulmonar.
IntroduçãoA hipertensão pulmonar é uma síndrome comum que engloba um amplo espectro de condições que às vezes têm patogênese semelhante, resultando em aumento da resistência vascular pulmonar, sobrecarga e disfunção ventricular direita e eventualmente óbito. A utilização de medicamentos para hipertensão pulmonar recentemente aprovados tem levado à melhora da capacidade funcional e da sobrevida dos pacientes com hipertensão pulmonar. Contudo, esse aumento da sobrevida cria desafios clínicos relacionados ao aumento da incidência de complicações crônicas.
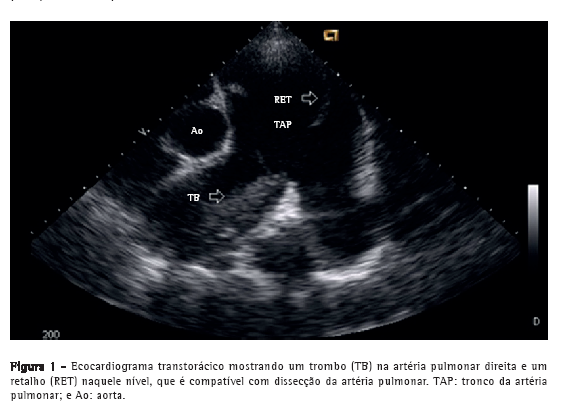
Relato de casoPaciente do sexo masculino, 50 anos, diagnosticado há quatro anos com hipertensão pulmonar relacionada à esquistossomose mansoni, admitido na emergência do Hospital das Clínicas da Faculdade de Medicina da Universidade Federal de Minas Gerais, localizado em Belo Horizonte, Brasil. Apresentava dor torácica retroesternal de início recente com agravamento progressivo e falta de ar (hipertensão pulmonar classe funcional III, de acordo com a Organização Mundial de Saúde). Havia sido diagnosticado com leucemia mieloide crônica há sete meses e estava em quimioterapia desde então. No momento da internação, o ecocardiograma transtorácico mostrava um grande trombo central não obstrutivo na artéria pulmonar principal direita. O átrio direito estava dilatado, e havia regurgitação tricúspide leve, com pressão sistólica em artéria pulmonar estimada em 63 mmHg. Foi diagnosticado como portador de trombose in situ como complicação de hipertensão pulmonar de longa duração. Após a possibilidade de síndrome coronária aguda ter sido excluída, recebeu alta em uso de varfarina. Foi reinternado dois meses depois em razão de dor torácica refratária com agravamento progressivo. Na época, apresentava SpO2 de 96%, e uma terceira bulha era audível no espaço paraesternal esquerdo inferior, acompanhada por murmúrio de regurgitação tricúspide. Os pulmões estavam limpos, e os pulsos arteriais periféricos estavam simétricos. Os exames laboratoriais estavam normais, incluindo os níveis séricos de creatinoquinase, creatinoquinase isoenzima MB e troponina. O eletrocardiograma de repouso evidenciava isquemia miocárdica aguda nas derivações anteriores. O ecocardiograma Doppler transtorácico revelava pressão sistólica da artéria pulmonar de 62 mmHg, um trombo na artéria pulmonar direita, como no exame anterior, e a presença de um retalho naquele nível que era compatível com dissecção da artéria pulmonar (Figura 1). O diagnóstico foi subsequentemente confirmado por angiografia pulmonar por TC (APTC; Figura 2). O paciente foi transferido para outro centro de tratamento cardiovascular, onde foram realizadas tentativas de correção do defeito por meio de um procedimento endovascular (através da veia femoral). No período perioperatório, o paciente apresentou choque cardiogênico refratário. Todos os esforços para reanimar o paciente foram infrutíferos, e ele faleceu na sala de cirurgia.
 Discussão
DiscussãoA dilatação aneurismática do tronco da artéria pulmonar e de seus ramos é uma condição conhecida que é amplamente relatada na literatura. Ocorre em consequência da hipertensão pulmonar de longa duração, sendo que a maioria dos casos relatados tem sido diagnosticada em autópsias.(1) Os primeiros relatos dessa condição em pacientes com esquistossomose vieram do Egito (em pacientes com esquistossomose hematóbica ou mansoni), seguidos, muito mais tarde, por relatos do Brasil (exclusivamente em pacientes com esquistossomose mansoni).(2,3) A dissecção da artéria pulmonar parece estar relacionada à dilatação da artéria pulmonar, inflamação da íntima, trombose in situ e aumentos agudos da pressão pulmonar.(4,5) A dilatação da artéria pulmonar e o aneurisma pulmonar têm sido relatados como fatores de risco que também estão associados a outras complicações.(4)
Até onde sabemos, este é apenas o segundo relato de um caso de dissecção da artéria pulmonar em paciente com hipertensão pulmonar relacionada à esquistossomose, sendo que o primeiro caso foi diagnosticado em autópsia.(6) Clinicamente, esses casos apresentam agravamento de sintomas anteriores de dispneia e dor torácica. A dor torácica é normalmente acentuada e pode simular síndrome coronariana aguda ou dissecção aguda da aorta. Cianose pode estar presente.(7) O diagnóstico é muitas vezes obtido post mortem, pois a maioria dos pacientes morre subitamente em razão de tamponamento cardíaco ou sangramento pulmonar grave. Se o diagnóstico é feito ante mortem, o primeiro achado é a emergência de um retalho na luz da artéria ou tronco pulmonar dilatado que se forma a partir da camada da íntima, denotando o orifício de entrada da falsa luz, mas raramente uma saída, que é o oposto do que é encontrado em casos de dissecção aórtica.(8) A ressonância magnética ou a APTC de tórax podem confirmar o diagnóstico e as complicações associadas, como aumento da dilatação da artéria pulmonar, sangue no líquido pleural e opacidades pulmonares.(1) A evolução é geralmente a ruptura do vaso com sangue se espalhando para o mediastino, pericárdio ou pulmão, pois não há saída da falsa luz. O orifício intimal que leva à dissecção ocorre no ponto de maior dilatação como consequência de um aumento da tensão parietal. Há relatos de que a inflamação causada por trombose in situ pode desempenhar um papel sinérgico no desenvolvimento da ruptura intimal.(4,9,10)
Embora seja razoável pensar que o diagnóstico e o tratamento precoces da hipertensão pulmonar adiariam a dissecção da artéria pulmonar, não há evidências que confirmem isso na literatura sobre o assunto, a qual consiste exclusivamente de revisões e relatos de caso. As opções terapêuticas são limitadas. A correção cirúrgica e o transplante de coração-pulmão são os procedimentos de escolha, mas ainda não são amplamente empregados, e, portanto, a quantidade de dados disponíveis é pequena.(7)
O aparecimento de uma dor torácica aguda ou nova, choque cardiogênico ou morte súbita em pacientes portadores de hipertensão pulmonar deve alertar para o diagnóstico de dissecção da artéria pulmonar.
Referências1. Moraes MG, Comparato LFL, Madi K. Aneurisma de artéria pulmonar: relato de um caso. Rev Med HSE. 1974;26(2):109-15
2. Zaky HA. Aneurysm of the pulmonary artery due to schistosomiasis. Dis Chest. 1952;21(2):194-204.
3. Santiago JM, Barros J, Rocha LF, Kalil M, Malleta CA, Chuster M. Aneurisma de artéria pulmonar secundário à hipertensão esquistossomótica. Relato de um caso. Arq Bras Cardiol. 1974;27(6):733-6.
4. Degano B, Prevot G, Têtu L, Sitbon O, Simonneau G, Humbert M. Fatal dissection of the pulmonary artery in pulmonary arterial hypertension. Eur Respir Rev. 2009;18(113):181-5.
5. Inayama Y, Nakatani Y, Kitamura H. Pulmonary artery dissection in patients without underlying pulmonary hypertension. Histopathology. 2001;38(5):435-42. Erratum in: Histopathology. 2001;39(5):550.
6. Miziara HL, Filomeno AP, Yunes MA. Dissecting aneurysm of the pulmonary artery, associated with pulmonary schistosomiasis. Report of a case [Article in Portuguese]. Arq Bras Cardiol. 1981;37(2):107-10.
7. Senbaklavaci O, Kaneko Y, Bartunek A, Brunner C, Kurkciyan E, Wunderbaldinger P, et al. Rupture and dissection in pulmonary artery aneurysms: incidence, cause, and treatment--review and case report. J Thorac Cardiovasc Surg. 2001;121(5):1006-8.
8. Song EK, Kolecki P. A case of pulmonary artery dissection diagnosed in the Emergency Department. J Emerg Med. 2002;23(2):155-9.
9. Moser KM, Fedullo PF, Finkbeiner WE, Golden J. Do patients with primary pulmonary hypertension develop extensive central thrombi? Circulation. 1995;91(3):741-5.
10. Andrews R, Colloby P, Hubner PJ. Pulmonary artery dissection in a patient with idiopathic dilatation of the pulmonary artery: a rare cause of sudden cardiac death. Br Heart J. 1993;69(3):268-9.
Trabalho realizado no Serviço de Pneumologia e Cirurgia Torácica, Hospital das Clínicas, Faculdade de Medicina, Universidade Federal de Minas Gerais, Belo Horizonte, Brasil.
Endereço para correspondência: Ricardo de Amorim Corrêa. Rua Abadessa Gertrudes Prado, 77 apto. 802, Vila Paris, CEP 30380-790, Belo Horizonte, MG, Brasil.
Tel. 55 31 3293-3910. E-mail: racorrea9@gmail.com
Apoio Financeiro: Nenhum.
Recebido para publicação em 2/7/2012. Aprovado, após revisão, em 7/12/2012.
Sobre os autoresRicardo de Amorim Corrêa
Professor. Serviço de Pneumologia e Cirurgia Torácica, Hospital das Clínicas, Faculdade de Medicina, Universidade Federal de Minas Gerais, Belo Horizonte, Brasil.
Luciana Cristina dos Santos Silva
Professora. Departamento de Medicina Interna, Faculdade de Medicina, Universidade Federal de Minas Gerais, Belo Horizonte, Brasil.
Cláudia Juliana Rezende
Chefe. Centro de Diagnóstico por Imagem, Hospital Madre Teresa, Belo Horizonte, Brasil.
Rodrigo Castro Bernardes
Chefe. Serviço de Cirurgia Cardiovascular, Hospital Madre Teresa, Belo Horizonte, Brasil.
Tarciane Aline Prata
Pneumologista. Serviço de Pneumologia e Cirurgia Torácica, Hospital das Clínicas, Faculdade de Medicina, Universidade Federal de Minas Gerais, Belo Horizonte, Brasil.
Henrique Lima Silva
Médico. Departamento de Medicina Interna, Hospital das Clínicas, Faculdade de Medicina, Universidade Federal de Minas Gerais, Belo Horizonte, Brasil.












 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket