
Continuous and bimonthly publication
ISSN (on-line): 1806-3756



Eduardo Sperb Pilla, Raôni Bins Pereira, Luiz Alberto Forgiarini Junior, Luiz Felipe Forgiarini,Artur de Oliveira Paludo, Jane Maria Ulbrich Kulczynski, Paulo Francisco Guerreiro Cardoso,Cristiano Feijó Andrade
ABSTRACT
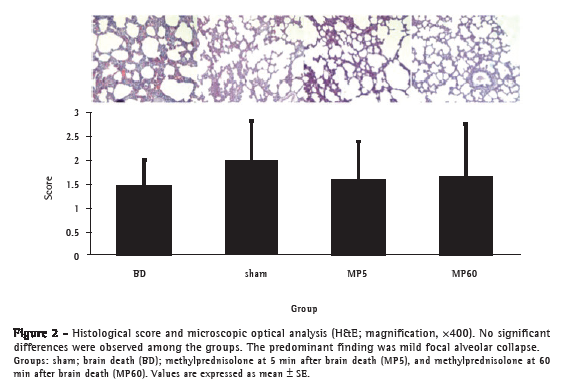
Objective: To evaluate the effects that early and late systemic administration of methylprednisolone have on lungs in a rat model of brain death. Methods: Twenty-four male Wistar rats were anesthetized and randomly divided into four groups (n = 6 per group): sham-operated (sham); brain death only (BD); brain death plus methylprednisolone (30 mg/kg i.v.) after 5 min (MP5); and brain death plus methylprednisolone (30 mg/kg i.v.) after 60 min (MP60). In the BD, MP5, and MP60 group rats, we induced brain death by inflating a balloon catheter in the extradural space. All of the animals were observed and ventilated for 120 min. We determined hemodynamic and arterial blood gas variables; wet/dry weight ratio; histological score; levels of thiobarbituric acid reactive substances (TBARS); superoxide dismutase (SOD) activity; and catalase activity. In BAL fluid, we determined differential white cell counts, total protein, and lactate dehydrogenase levels. Myeloperoxidase activity, lipid peroxidation, and TNF-α levels were assessed in lung tissue. Results: No significant differences were found among the groups in terms of hemodynamics, arterial blood gases, wet/dry weight ratio, BAL fluid analysis, or histological score-nor in terms of SOD, myeloperoxidase, and catalase activity. The levels of TBARS were significantly higher in the MP5 and MP60 groups than in the sham and BD groups (p < 0.001). The levels of TNF-α were significantly lower in the MP5 and MP60 groups than in the BD group (p < 0.001). Conclusions:áIn this model of brain death, the early and late administration of methylprednisolone had similar effects on inflammatory activity and lipid peroxidation in lung tissue.
RESUMO
Objetivo: Avaliar os efeitos da administração sistêmica precoce e tardia de metilprednisolona nos pulmões em um modelo de morte encefálica em ratos. Métodos: Vinte e quatro ratos Wistar machos foram anestesiados e randomizados em quatro grupos (n = 6 por grupo): sham, somente morte encefálica (ME), metilprednisolona i.v. (30 mg/kg) administrada 5 min após a morte encefálica (MP5) e 60 min após a morte encefálica (MP60). Os grupos ME, MP5 e MP60 foram submetidos à morte encefálica por insuflação de um balão no espaço extradural. Todos os animais foram observados e ventilados durante 120 min. Foram determinadas variáveis hemodinâmicas e gasométricas, relação peso úmido/seco, escore histológico, thiobarbituric acid reactive substances (TBARS, substâncias reativas ao ácido tiobarbitúrico), atividade de superóxido dismutase (SOD) e de catalase, assim como contagem diferencial de células brancas, proteína total e nível de desidrogenase lática no LBA. A atividade da mieloperoxidase, peroxidação lipídica e níveis de TNF- foram avaliados no tecido pulmonar. Resultados: Não foram observadas diferenças significativas nas variáveis hemodinâmicas e gasométricas, relação peso úmido/seco, análises do LBA, escore histológico, SOD, mieloperoxidase e catalase entre os grupos. Os níveis de TBARS foram significativamente maiores nos grupos MP5 e MP60 do que nos grupos sham e ME (p < 0,001). Os níveis de TNF- foram significativamente menores nos grupos MP5 e MP60 do que no grupo ME (p < 0,001). Conclusões: Neste modelo de morte cerebral, a administração precoce e tardia de metilprednisolona apresentou efeitos semelhantes sobre a inflamação e a peroxidação lipídica no tecido pulmonar.
Palavras-chave: Ratos; Morte encefálica; Estresse oxidativo; Pulmão; Hidroxicorticosteroides.
Introduction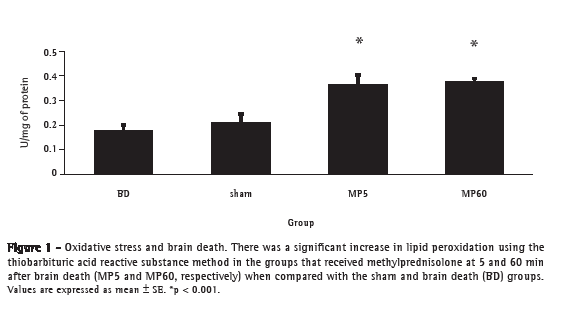



Sociedade Brasileira de Pneumologia e Tisiologia
Secretaria do Jornal Brasileiro de Pneumologia
SCS Quadra 01, Bloco K, Salas 203/204 Ed. Denasa
Brasília - DF CEP: 70.398-900
Fone/fax: 08000 61 6218, (61) 3245 1030 e (61) 3245 6218
E-mail: jbp@sbpt.org.br
Development by: ![]()
© All rights reserved 2025 - Jornal Brasileiro de Pneumologia
 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket




